

9 YEAR MALE CHILD, C/O- LEFT WRIST DROP, MILD SHARP PAIN OF HUMERUS DUE TO INJURY 8 MONTHS BACK, TO ASSESS FOR RADIAL NERVE INJURY
HISTORY
- 9 YEAR MALE CHILD, C/O- LEFT WRIST DROP, MILD SHARP PAIN OF HUMERUS DUE TO INJURY 8 MONTHS BACK, TO ASSESS FOR RADIAL NERVE INJURY
- MRI LEFT ARM WITH FORARM ADVISED.
FINDINGS
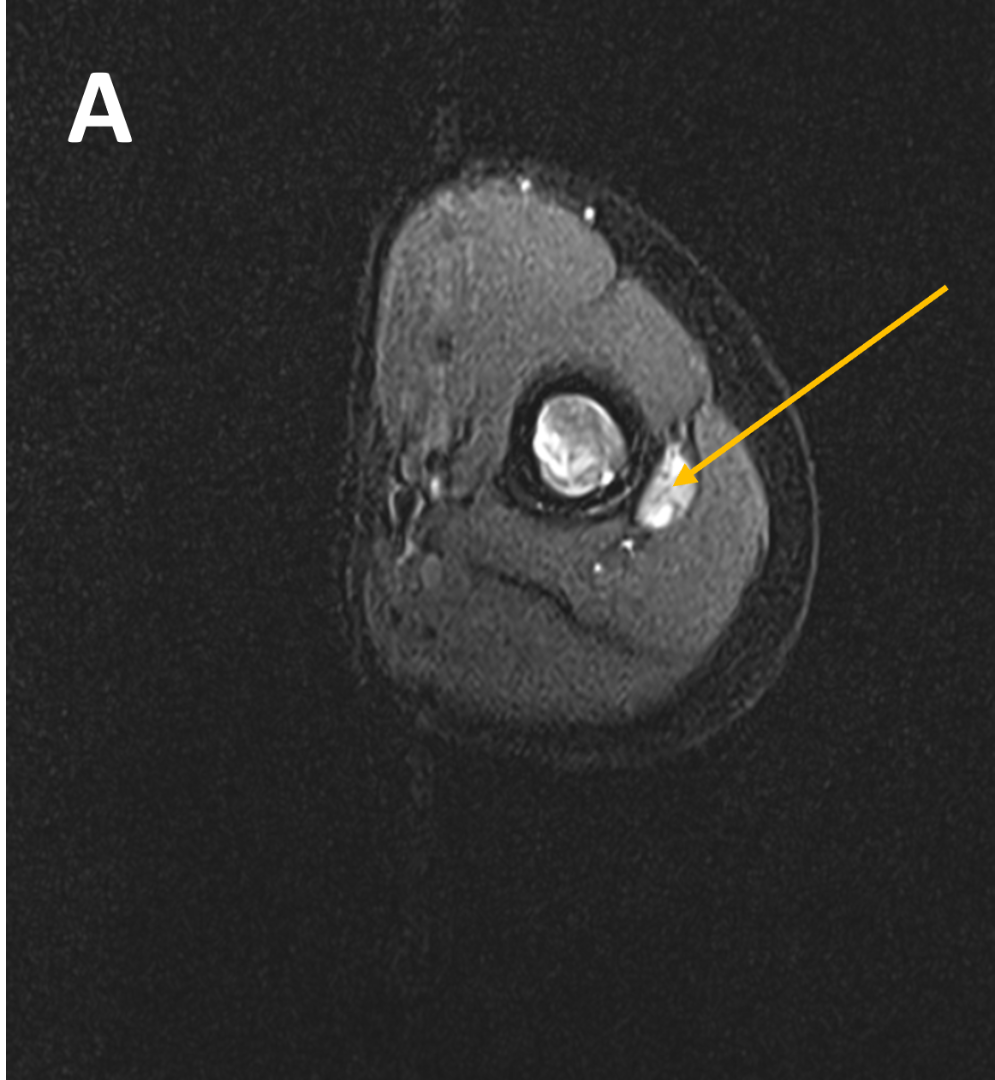
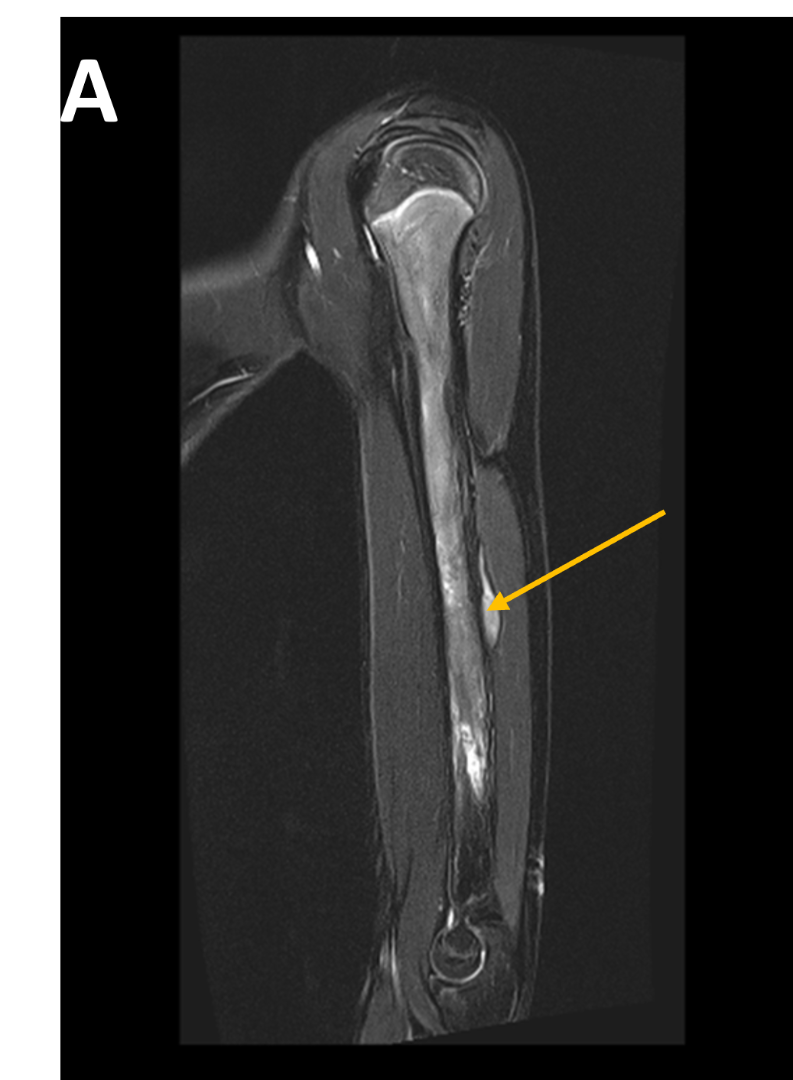
- (A,B) : MR LEFT FOREARM
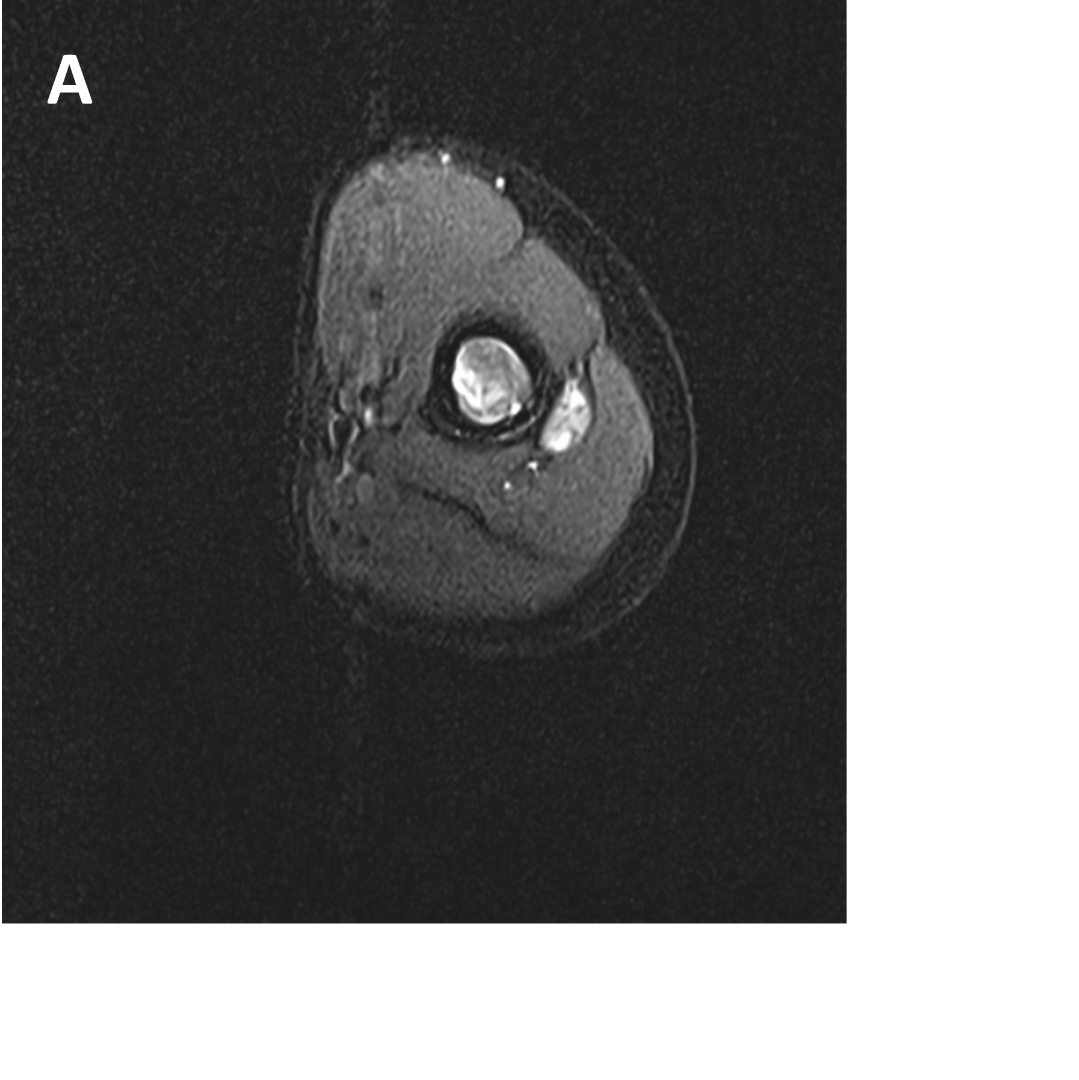
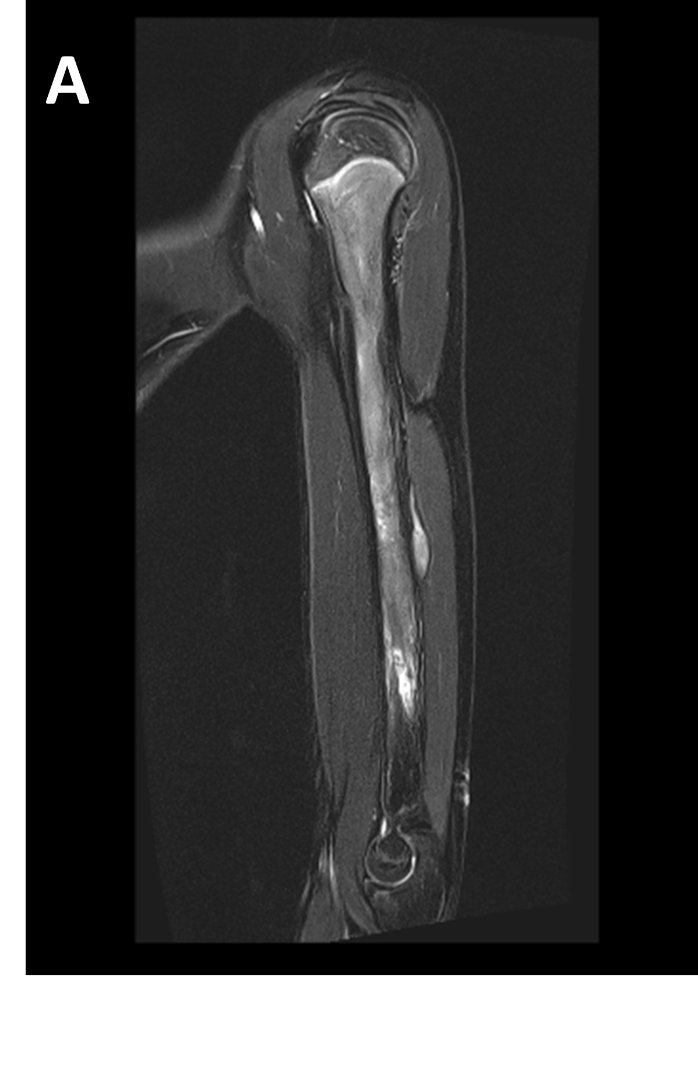

- A : MR LEFT FOREARM : Fusiform thickening of radial nerve in the posterior compartments of mid-distal 1/3rd arm, as its winds around the spiral groove of the humerus, before piercing the lateral intermuscular septum.
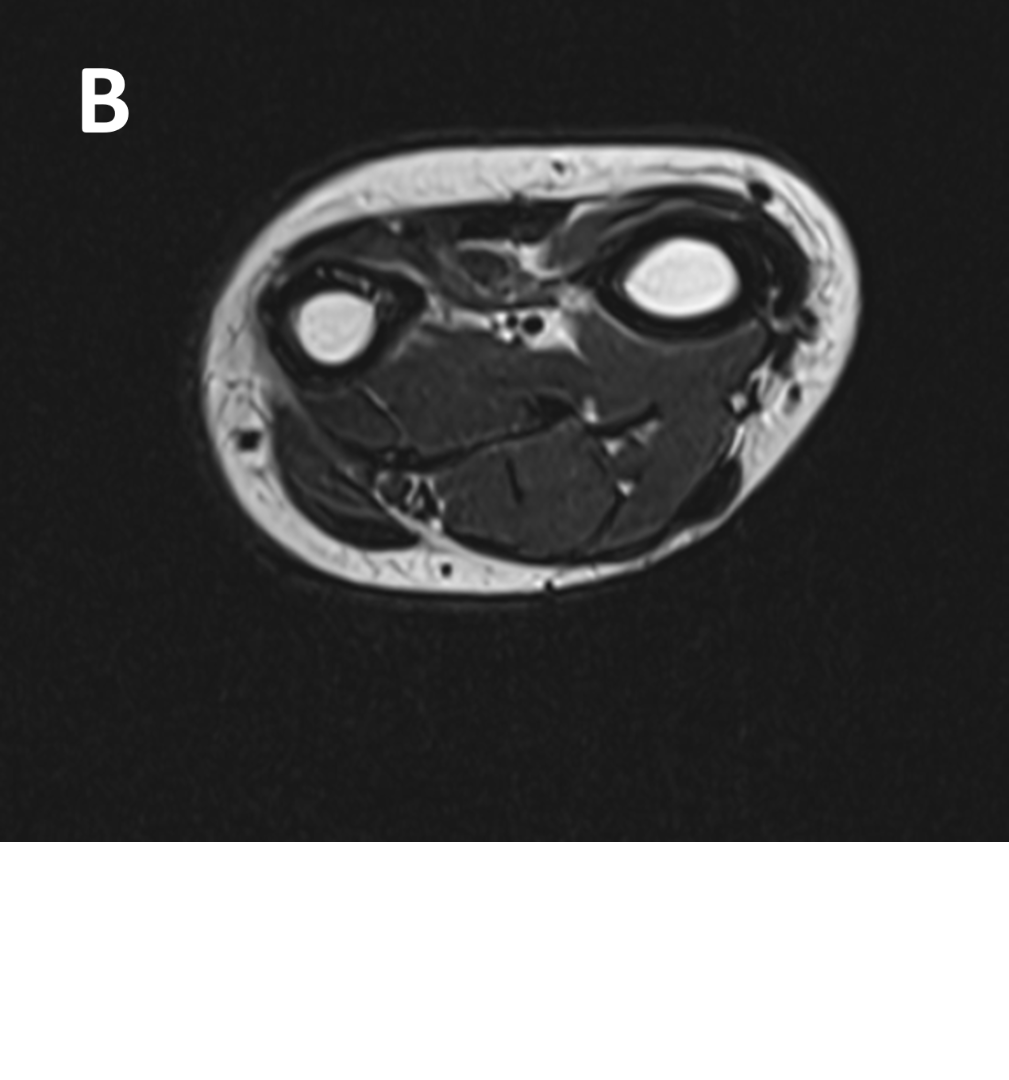
- B 1 : Tract of previous intramedullary nail seen in shaft of humerus, along with mild diffuse cortical thickening.
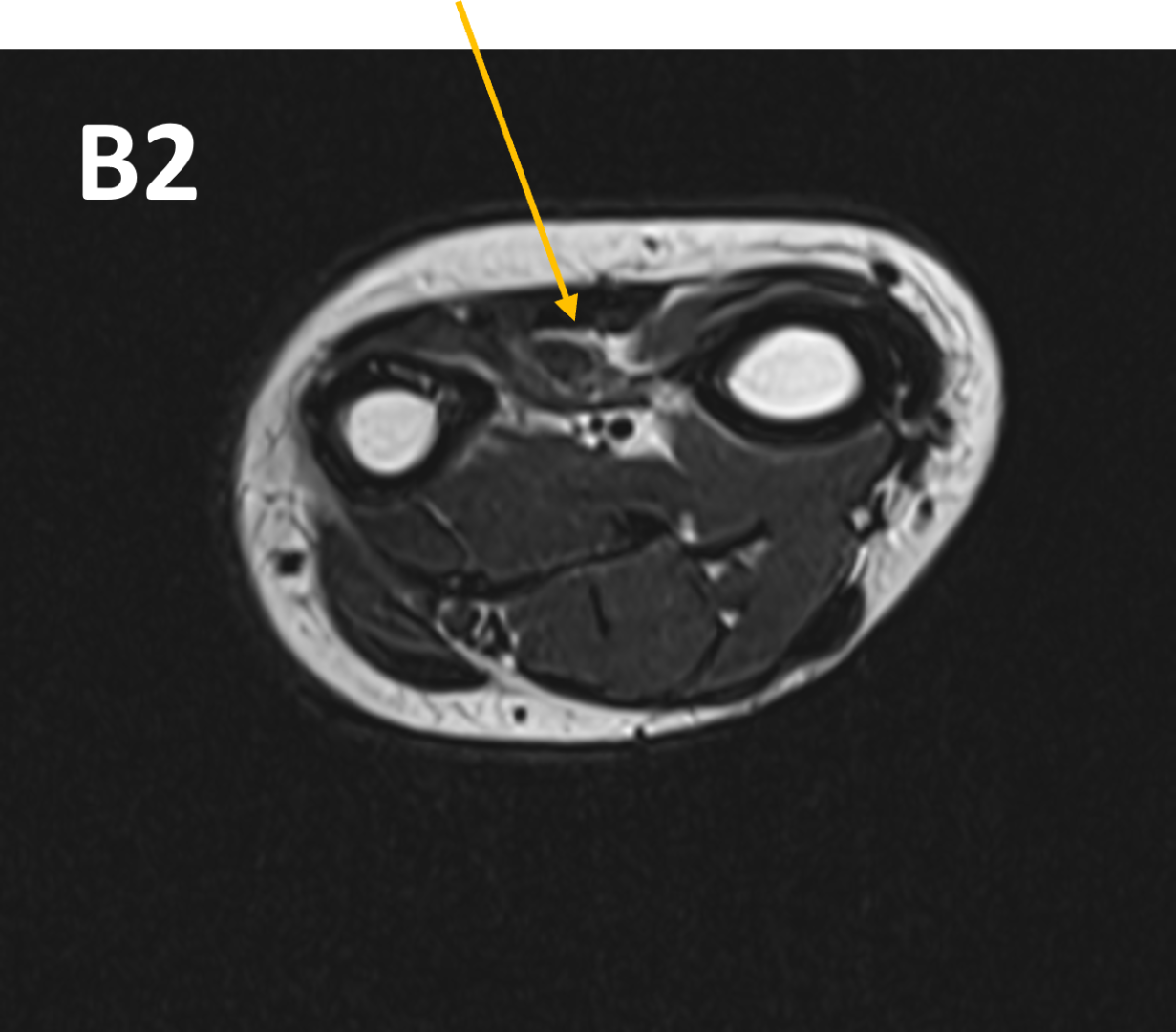
- B 2 : Volume loss with fatty atrophy of brachioradialis, supinator, extensor carpi radialis longus and brevis muscles ,due to chronic denervation changes.

DIAGNOSIS
- POST TRAUMATIC NEUROMA OF RADIAL NERVE WITH DENERVATION CHANGES
DISCUSSION
- Pathophysiology
- Traumatic injury (laceration, transection, traction, crush) → axonal disruption
- Aberrant repair: Axons attempt regeneration but grow in disorganized, multidirectional fashion
- Result: Focal enlargement with loss of normal fascicular architecture
Two Types of Traumatic Neuroma
- Spindle Neuroma
- Nerve trunk intact but injured
- Fusiform (spindle-shaped) swelling at injury site
- Continuous with proximal & distal segments
- Terminal Neuroma
- Nerve avulsed/transected (complete disruption)
- Bulbous enlargement at end of proximal stump
- No distal segment visible
Clinical Presentation
- Timeline after injury:
- Most common: 1 month to 12 months post-injury
- Can occur as early as 8 days or as late as 40 years
- Symptoms & Signs:
- Pain (20-30% of neuromas are painful; mild to incapacitating)
- Palpable mass at site of prior trauma
- Tinel's sign: Percussion of mass elicits pain/tingling
- Temporary relief with local anesthetic injection (diagnostic)
Management & Prognosis
- Asymptomatic (most common):
- Observation; no treatment needed
- Symptomatic:
- Local anesthetic injection (diagnostic & therapeutic)
- Neuroma debulking/excision (surgical)
- Nerve repair if feasible (depends on injury type)
- Note: Traumatic neuroma is benign and does NOT transform to malignancy
REFERENCES
- Traumatic Neuroma- RadSource MRI Web Clinic. : https://radsource.us/traumatic-neuroma/
- StatPearls-Traumatic Neuroma. : https://www.ncbi.nlm.nih.gov/books/n/statpearls/article-25808/
- Rhoul et al. Post-Traumatic Radial Nerve Neuroma (Case Report). : https://pubmed.ncbi.nlm.nih.gov/37601552/
- MRI Features of Peripheral Traumatic Neuromas. : https://pubmed.ncbi.nlm.nih.gov/26188658/
DR. KAMESH G
CONSULTANT RADIOLOGIST
MANIPAL HOSPITAL, YESHWANTHPUR
DR.FATHIMATH ASHILI KM
RADIOLOGY RESIDENT
MANIPAL HOSPITAL, YESHWANTHPUR

