
86-year-old female with history of hypertension since 1 year came with the complaints of – abdomen pain with swelling, vomiting, constipation and fever of 10 days.
- 86-year-old female with history of hypertension since 1 year came with complaints of – abdomen pain with swelling, vomiting, constipation and fever of 10 days. ?
- USG shows cholelithiasis with? SAIO.?
- Patient underwent CECT abdomen which shows.
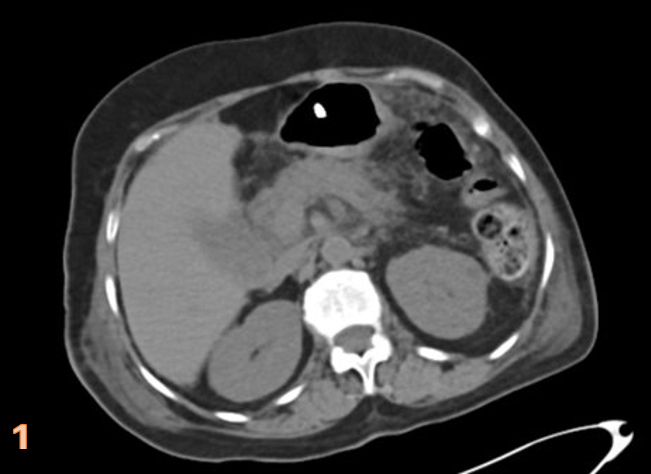


PANCREAS:
- non-enhancing low attenuating regions within the pancreas suggestive of areas of necrosis(arrows) (fig. 1). ?
- edematous pancreas.
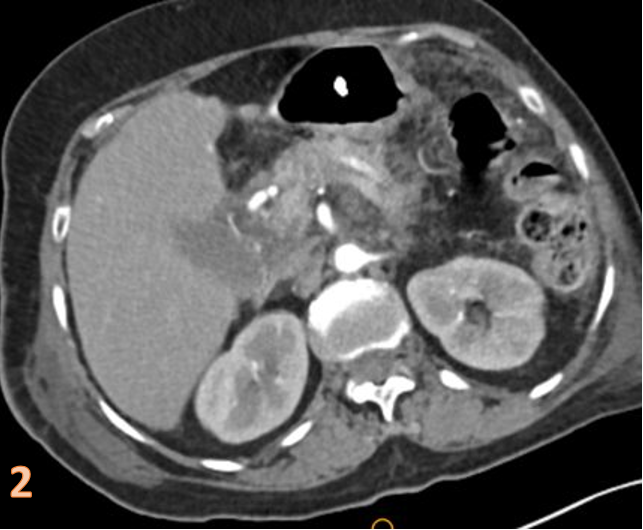
PERIPANCREATIC TISSUE (fig.2-3):
- Peripancreatic fat stranding and fluid collection (*).?
- multiple enhancing nodular lesions of small size dispersed at omentum, peripancreatic, mesenteric and pericholecystic region(arrows).?
- Bilateral anterior pararenal fascia and lateral conal fascia thickening (arrowhead).
EXTRAPANCREATIC COMPLICATIONS-?(fig.3-4):
- Bilateral pleural effusion with collapse and consolidation of underlying bilateral lower lung lobes more on left side (+).?
- Grossly enlarged gall bladder with pericholecystic fat stranding and mild reactive wall thickening (curved arrow).
DIAGNOSIS:
FAT SAPONIFICATION in ACUTENECROTICBILIARY PANCREATITIS
CLINICAL SIGNIFICANCE:
- The presence of scattered nodular lesions in the omentum are commonly seen in and attributed to malignancies such as primary/ secondary peritoneal carcinomatosis, tuberculosis or peritoneal lymphomatosis, particularly in the elderly
- This case highlights a less common but clinically significant association of omental and retroperitoneal nodularity in pancreatitis secondary to fat saponification.
- It also reflects the importance of vetting clinical information which can prove to be crucial in pointing towards a more acute and benign etiology.
DISCUSSION
POST-PANCREATITIS FAT SAPONIFICATION(3)
- In pathophysiology of acute pancreatitis, there is release of pancreatic enzymes which are responsible for provoking a secondary systemic response. These include lipolytic enzymes that “self-digest” pancreatic tissue and peripancreatic fat.
- The lysis of the fat cells will cause the release of fatty acids that precipitate with the serum calcium in the form of soap. This is the phenomenon known as fatty saponification and is thought to be responsible for the hypocalcemia that is typically associated with severe acute pancreatitis.
- Radiological manifestations associated with the phenomenon of fatty saponificationusually appear after the resolution of ascites and exudate in the context of acute pancreatitis.
- The most characteristic feature is the presence of multiple nodular lesions of small size and dispersed at the mesenteric or retroperitoneal level which may have a mass effect and delayed enhancement after administration of intravenous contrast.
DIFFERENTIAL DIAGNOSIS(4)
Peritoneal carcinomatosis
- Peritoneal metastases are mainly seen in ovarian and gastric malignancies.
- Smooth or nodular thickening of the peritoneum and leaves of the mesentery is the most characteristic presentation along with peritoneal enhancement. A stellate appearance of the mesentery may be encountered. Invasion of the fat of the greater omentum with nodules, produces the renowned omental cake(Fig 5 ), black arrow heads).
- A moderate to large volume of ascites is also a frequent finding in peritoneal carcinomatosis. When features atypical of pancreatic fat saponification or mesenteric panniculitis are present or if the clinical history does not coincide with the imaging findings, peritoneal carcinomatosis should be included in the differential diagnosis.
 Peritoneal lymphomatosis
Peritoneal lymphomatosis
- Diffuse peritoneal involvement in lymphomatous disease is encountered above all-in high-grade lymphomas, lymphomas complicating AIDS, and Burkitt lymphomas.
- Tumour invasion of the greater omentum or mesentery and abnormal thickening of the peritoneal serous membrane may be seen (Fig. 6)
- Frequent lymph node involvement, associating preaortic and retroperitoneal lymphadenopathy. It appears as confluent masses encasing the mesenteric vasculature, producing the ‘‘sandwich’’ sign (Fig. 6). These masses are bulky, soft, non-obstructing, homogeneous without significant necrosis, and they seem to be less vascularised than carcinomatosis.
- Splenomegaly, although this is not always present.
- The presence of tumours in the gastrointestinal tract, especially the stomach and the terminal ileum.
 Peritoneal tuberculosis
Peritoneal tuberculosis
- Wet type comprises ascites (Fig 7, 8) with increased density due to their high protein content
- Regular thickening and enhancement of the peritoneal serous membrane. (Fig.8)
- Invasion of the mesentery and serous membrane of the greater omentum with macronodulespresent.
- Lymphadenopathy with or without a necrotic centre , black arrowhead), involvement of the ileocecal wall & Calcifications in the spleen.


References:
- Acute Pancreatitis: Revised Atlanta Classification and the Role of Cross-Sectional Imaging: Ken Zhao et al.
- https://radiopaedia.org/articles/acute-pancreatitis
- Post-pancreatitis fat saponification imitating carcinomatosis: M. J. Regaña Feijoó, T. Díaz Antonio, L. Dominguez Gomez, A. Ruiz Salas, A. Dominguez Igual, C. Leiva Vera; Malaga/ES
- Diop AD, et al. CT imaging of peritoneal carcinomatosis and its mimics. Diagnostic and Interventional Imaging (2014)
Dr Sunita Gopalan
DMRD, FRCR
Senior Consultant Radiologist
Columbia Asia Radiology Group
Dr Shashwat Priyadarshi,
MBBS DNB
Cross-sectional fellow
