
8 -year child presenting with headache and diminished vision.
8 -year child presenting with headache and diminished vision.
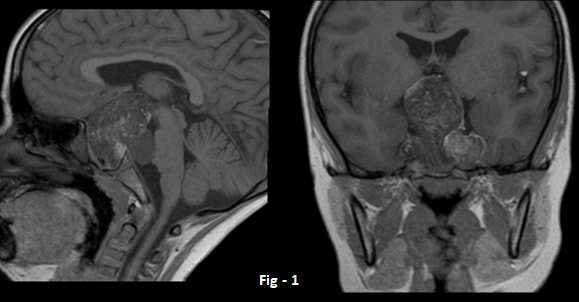
- Sagittal and Coronal T1 images demonstrate lobulated, predominantly hypointense lesion with multiple internal hyperintense areas (Blue and orange arrows) in sellar- suprasellar region. Hyperintense nodular foci also noted in left sylvian fissure (green arrows).
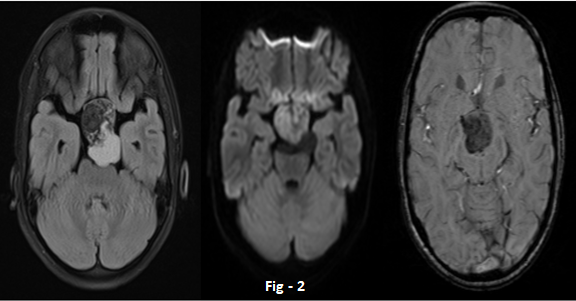
- Axial FLAIR image demonstrates suppression of right side of lesion (orange arrow) with few lobulated non suppressed component posteriorly (blue arrow). Axial DWI images demonstrate mild diffusion restriction. Axial GRE images demonstrates extensive areas of blooming within the lesion.
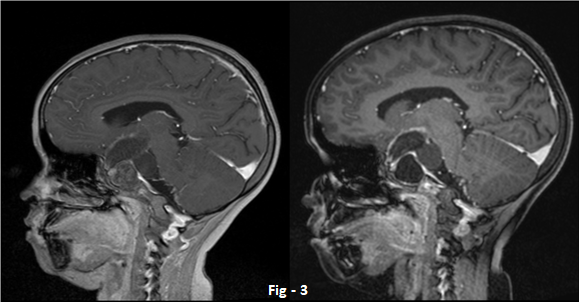
- Sagittal T1w postcontrast non fat sat and fat sat images demonstrate peripheral marginal enhancement (blue arrows) with a hyperintense content (orange arrow) suppressed on fat sat image (white arrow).
-
DIAGNOSIS:
Sellar-suprasellar dermoid with rupture.
DISCUSSION:
- Intracranial dermoid cysts are relatively rare, benign lesions. They are usually congenital and slow growing.
- Symptoms usually occur due to mass effect on adjacent intracranial structures.
- Rupture is an uncommon complication, can occur spontaneously or following closed head trauma or surgery.
- Rupture may result in chemical meningitis, vasospasm and cerebral infarction.
-
Case contributed by:
Dr. Sriram S Patwari MD, PDCC.
Consultant Radiologist and Co-lead Neuroradiology
Manipal Hospitals Radiology Group.Dr. Sushant Mittal
Cross sectional fellow
Manipal Hospitals Radiology Group.REFERENCES:
- Jacków J, Tse G, Martin A, S?siadek M, Romanowski C. Ruptured intracranial dermoid cysts: a pictorial review. Pol J Radiol. 2018;83:e465-e470. Published 2018 Oct 19. doi:10.5114/pjr.2018.80206
- Ray MJ, Barnett DW, Snipes GJ, Layton KF, Opatowsky MJ. Ruptured intracranial dermoid cyst. Proc (Bayl Univ Med Cent). 2012;25(1):23-25. doi:10.1080/08998280.2012.11928775
-
Differential diagnosis:
- Other lesions demonstrating T1 high signal eg haemoglobin degradation products, colloid cysts, craniopharyngioma and melanoma should be kept in differential diagnosis
- However fat suppression shall help in detecting fat component within the lesion and, hence pinpointing the diagnosis.
-
Imaging features are:
- Midline, usually sellar suprasellar mass lesion followed by posterior fossa.
- Typically, high signal on T1 images and heterogeneously hyperintense on FLAIR; chemical shift artifacts can be seen.
- T2*/ GRE images demonstrates blooming artifacts.
- Usually peripheral rim enhancement is noted, wall can also calcify and hence bloom.
- Ruptured dermoid cysts demonstrate T1 high signal intensity and blooming in subarachnoid spaces signifying disseminated fat droplets.
Dr. Sriram S Patwari MD, PDCC.
Consultant Radiologist and Co-lead Neuroradiology
Manipal Hospitals Radiology Group.
Dr. Sushant Mittal
Cross-sectional fellow
Manipal Hospitals Radiology Group.
