

77-year-old gentleman presented with abdominal pain and recent drop in hemoglobin.
A 77-year-old gentleman presented with abdominal pain and a recent drop in hemoglobin.



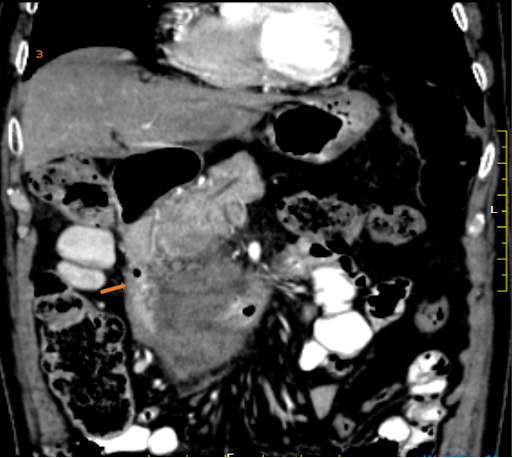
Triphasic CT and Correlative MRI ABDOMEN:
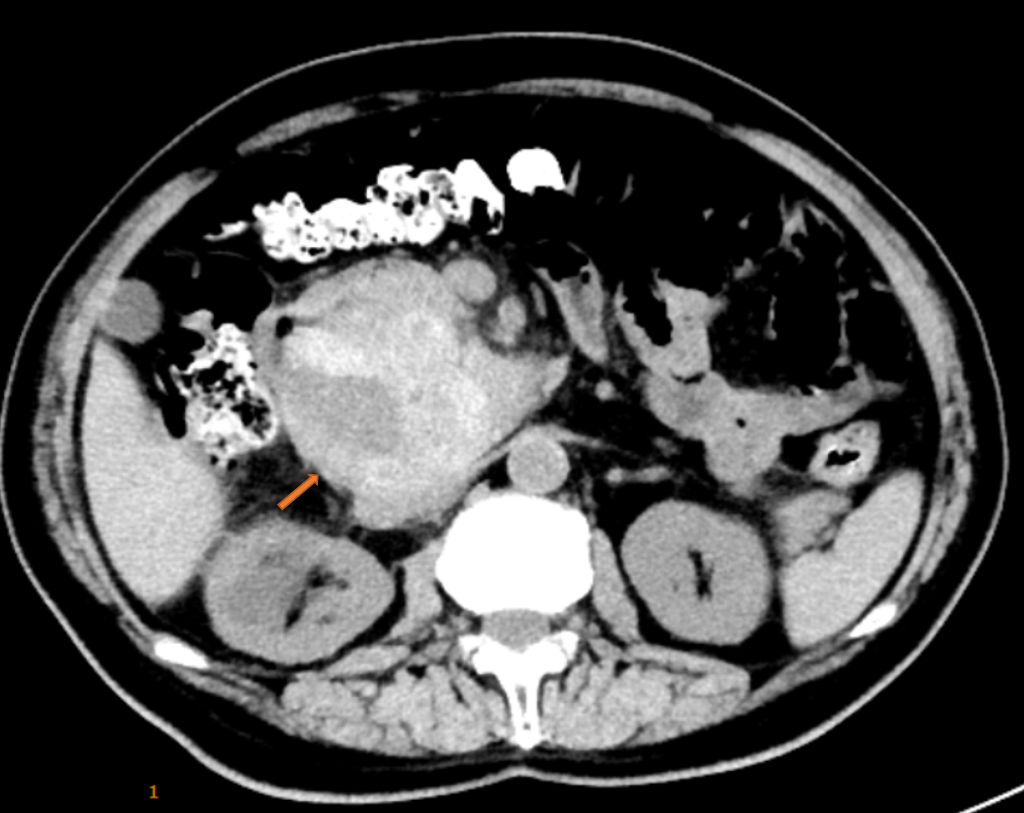
- There is a large lobulated retroperitoneal mass lesion in the Passaro’s Triangle with internal hyperdensity in keeping with hemorrhage. No calcification/ fat density within. It is displacing the 3rd and 4th part of the duodenum and head of the pancreas anterosuperior, displacing and compressing IVC inferomedial (Fig1)
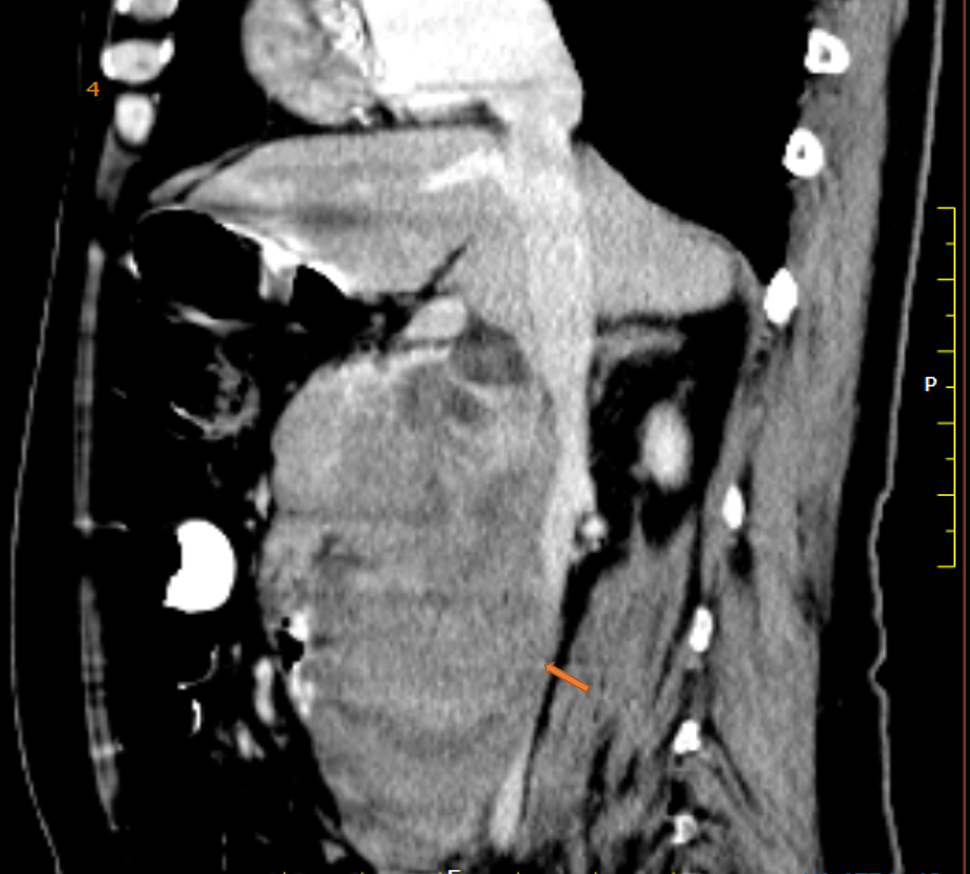
- There is early arterial rim hyperenhancement in the predominantly cystic superior component. (Fig 2 )
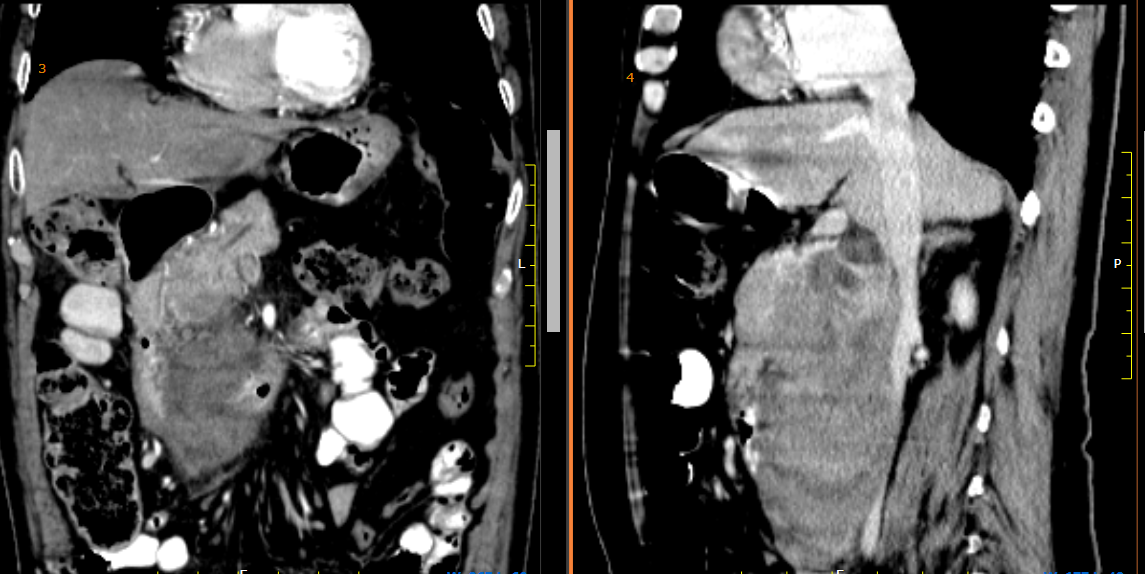
- The pancreatic duct is normal in caliber. There is a mass effect on the “C’ loop of the duodenum and the IVC and mild enhancement of the inferior solid component. (Fig 3 and 4)
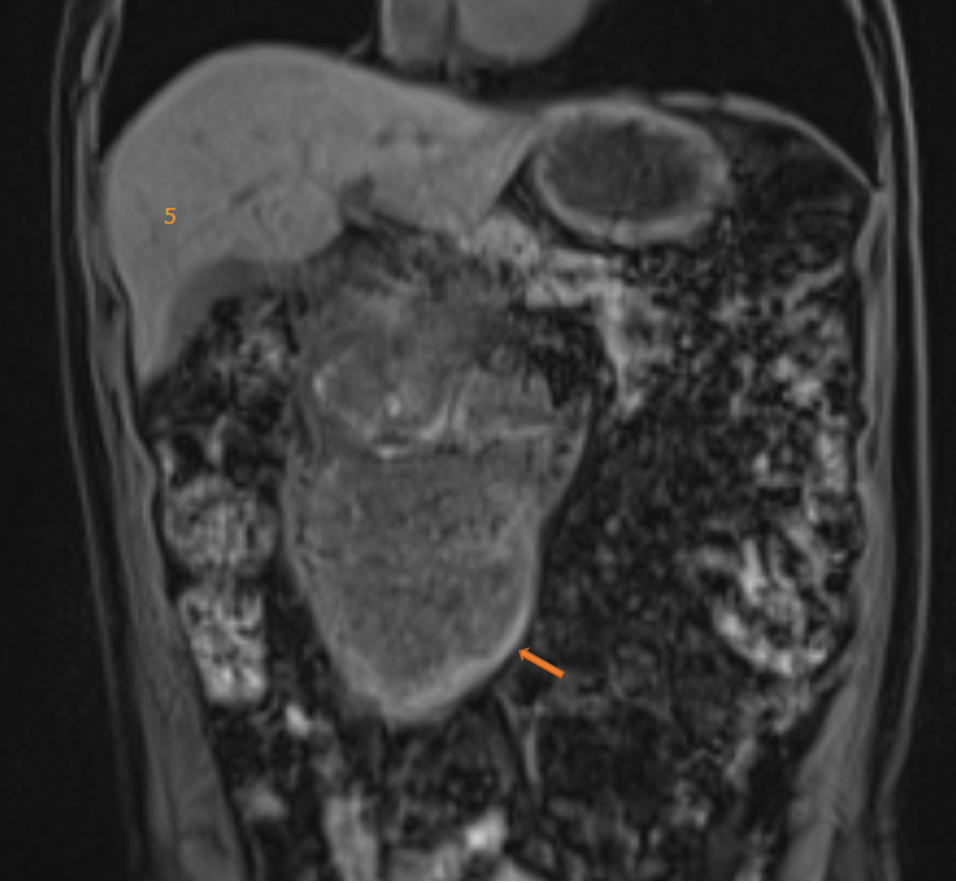
- The lesion is T1 hypointense with hyperintense rim ( Figure 5)
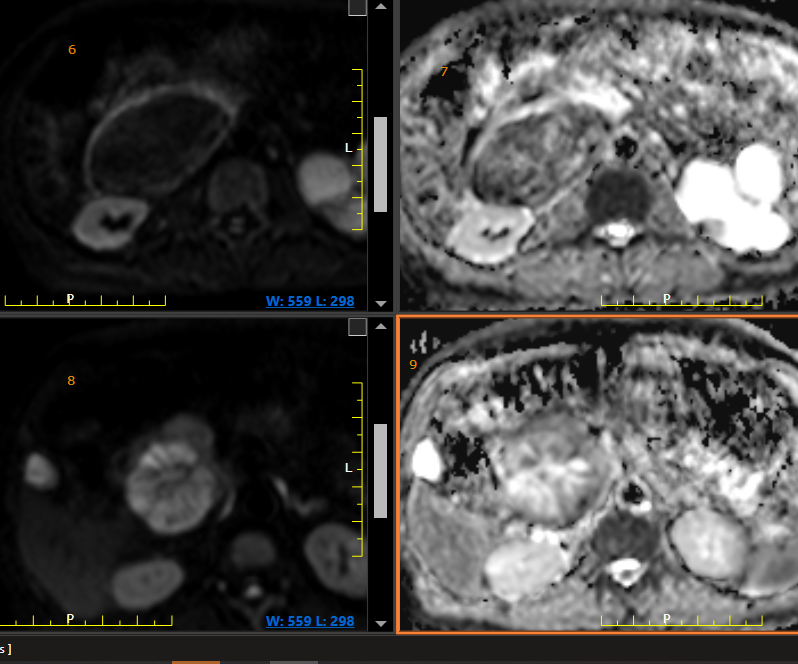
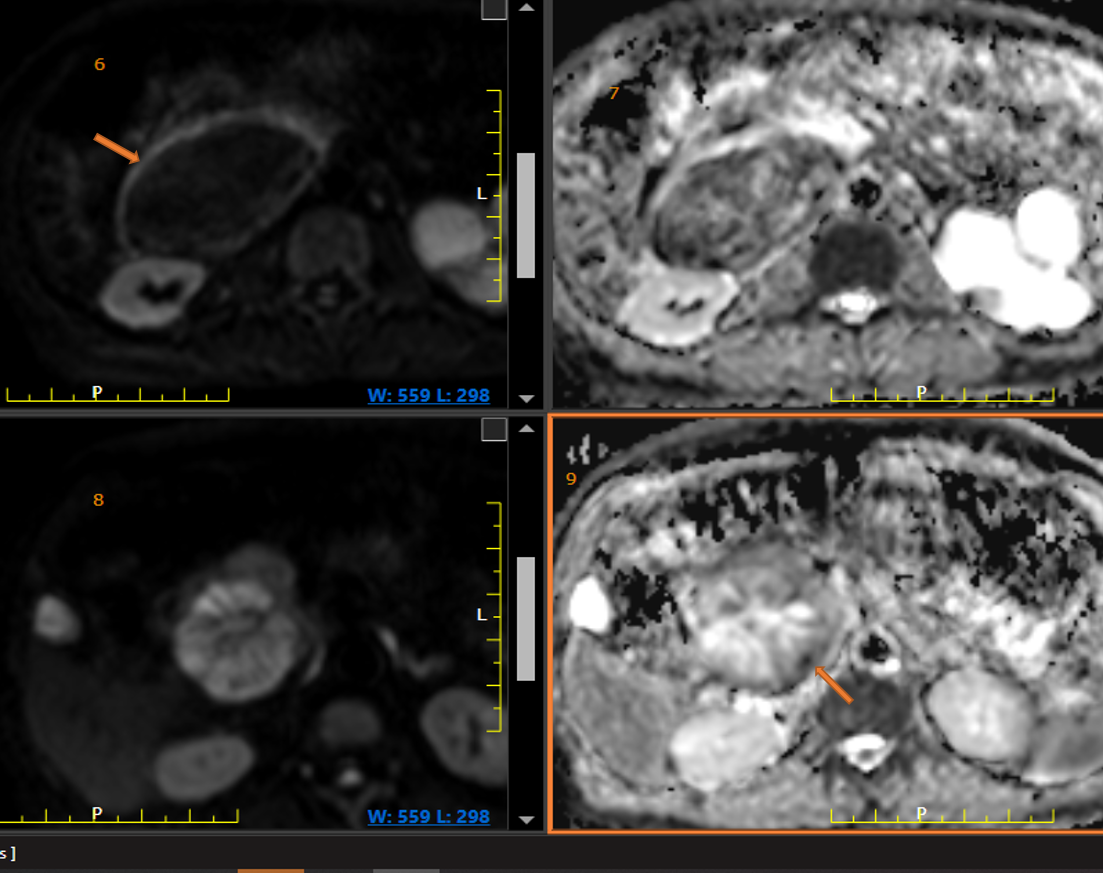
- The solid inferior component shows no restriction, except a peripheral rim (Fig6 and 7) and the cystic superior component shows T2 shine thru with some peripheral restriction (Fig 8 and 9).
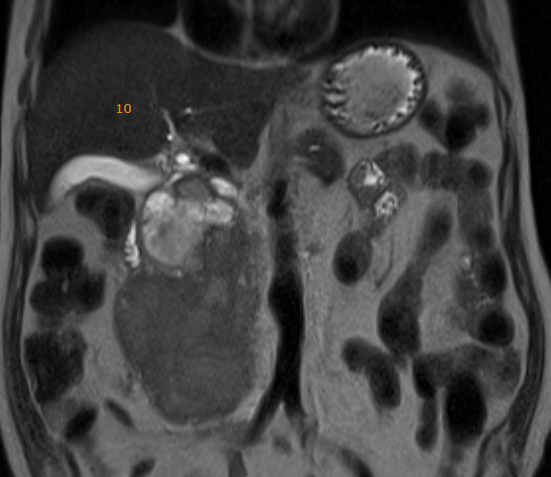
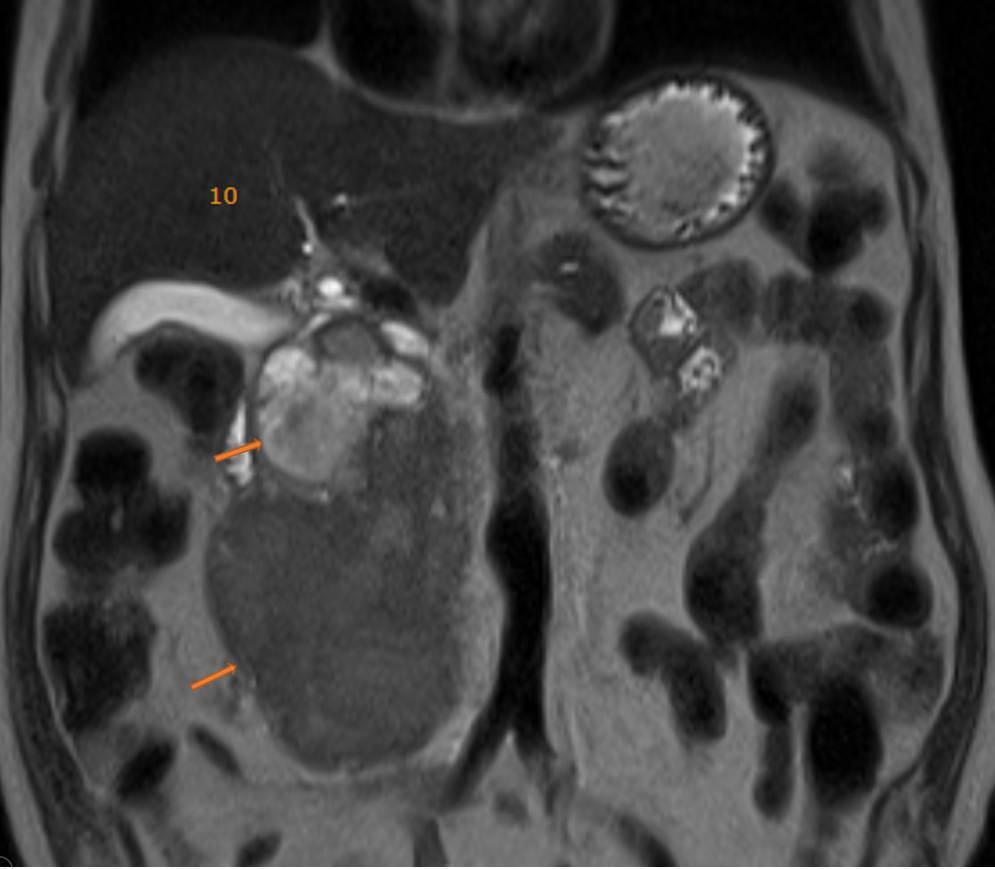
- On T2 the lesion is heterogeneous, with cystic superior and inferior solid components, No intrahepatic biliary duct dilatation. No liver lesions (Fig 10)
- Post-operative specimen with Hemorrhage (Fig.11).

DIAGNOSIS:
Well-differentiated (non-functioning) Neuroendocrine Tumor Grade 1 with internal hemorrhage of possible pancreatic origin.
DISCUSSION:
- Neuroendocrine tumors (NETs) are a large heterogeneous group of malignancies that are derived from embryonic neural crest tissue found in various organs.
- Neuroendocrine neoplasms arise in almost every organ of the body and are variably defined according to the site of origin.
- The 2017 WHO classification of tumors of the digestive system introduces grading and staging tools for neuroendocrine neoplasms.
- There are two genetically distinct neoplasms that include well-differentiated panNETs and poorly differentiated panNECs (small and large cell types)
- Currently, the term neuroendocrine tumor (NET) encompasses low to intermediate grade, well to moderately differentiated neoplastic lesions, whilst neuroendocrine carcinoma (NEC) refers to high-grade, moderately to poorly differentiated neoplastic lesions.
- The terminology for neuroendocrine lesions varies in different organs and includes adenoma or carcinoma in pituitary, parathyroid and thyroid glands (for medullary thyroid carcinoma only), pheochromocytoma and malignant pheochromocytoma in the adrenal glands (paraganglioma and malignant paraganglioma for extraadrenal paraganglia) and carcinoid and small-cell or large-cell carcinoma in the airway and digestive systems.
- Gastroenteropancreatic NETs (GEP?NETs) include carcinoid tumors of the gastrointestinal tract and pancreatic NETs (pNETs).
- Triple phase CT is the diagnostic modality of choice for initial evaluation and anatomic imaging of suspected NE neoplasms.
- However, functional Somatostatin receptor imaging with somatostatin analog radiotracers is the sole imaging modality that allows selection of patients for peptide receptor radionuclide therapy
REFERENCES:
- Pancreatic Neuroendocrine Neoplasms: 2020 Update on Pathologic and Imaging Findings and Classification, Lokesh Khanna, Srinivasa R. Prasad, Abhijit Sunnapwar, Sainath Kondapaneni, Anil Dasyam, Varaha S. Tammisetti, Umber Salman, Alia Nazarullah, and Venkata S. Katabathina, RadioGraphics 2020 40:5, 1240-1262
- Speel EJ, Richter J, Moch H et-al. Genetic differences in endocrine pancreatic tumor subtypes detected by comparative genomic hybridization. Am. J. Pathol. 1999;155 (6): 1787-94. doi:10.1016/S0002-9440(10)65495-8 – Free text at pubmed – Pubmed citation
- Rindi G, Leiter AB, Kopin AS et-al. The “normal” endocrine cell of the gut: changing concepts and new evidence. Ann. N. Y. Acad. Sci. 2004;1014: 1-12. Pubmed citation
- Rindi G, Wiedenmann B. Neuroendocrine neoplasms of the gut and pancreas: new insights. Nat Rev Endocrinol. 2011;8 (1): 54-64. doi:10.1038/nrendo.2011.120 – Pubmed citation
Dr. Sulagna Banerjee
MBBS, DNB (Radiodiagnosis)
Senior Consultant – Radiology
Columbia Asia Hospital, Sarjapur.
Dr. Sunita Gopalan
DMRD, FRCR
Senior Consultant Radiologist
Columbia Asia Radiology Group.
Dr Suvarna Kote, DMRD
Radiology resident
Columbia Asia Radiology Group.
