
A 71-year-old lady presented with left flank pain. She was a follow up case of adenocarcinoma lung– status post lobectomy, chemoradiation and currently on maintenance chemotherapy.
- Ultrasound revealed left sided hydronephrosis.
FINDINGS:
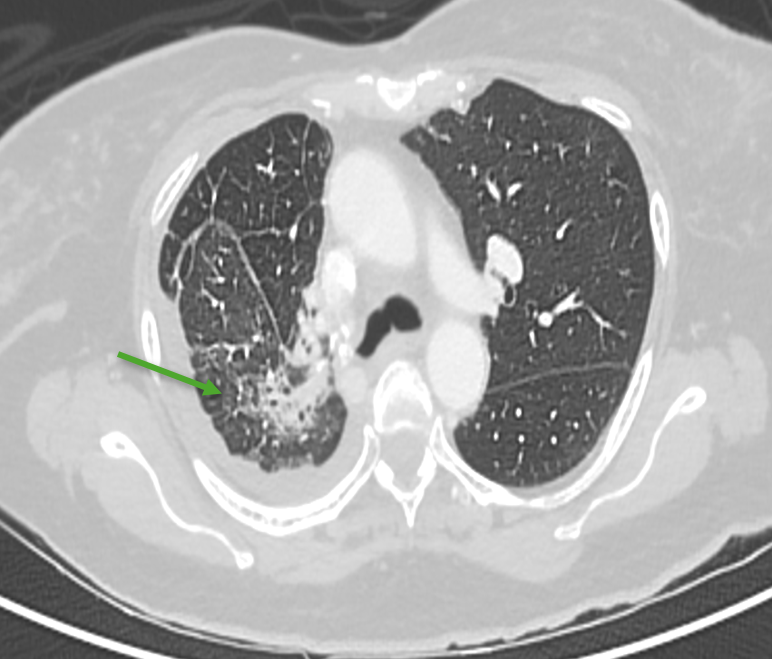
- Axial CT images of the chest in lung window.
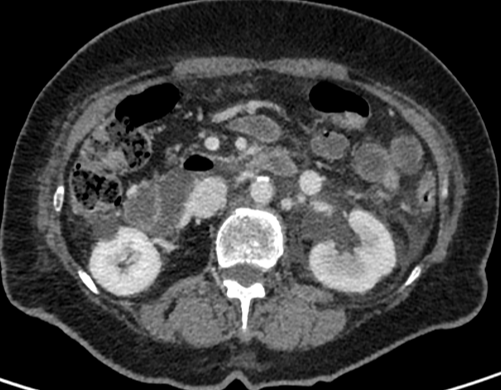
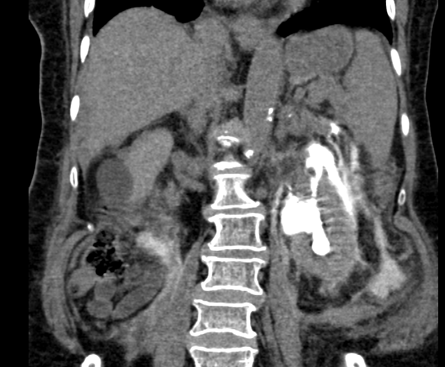
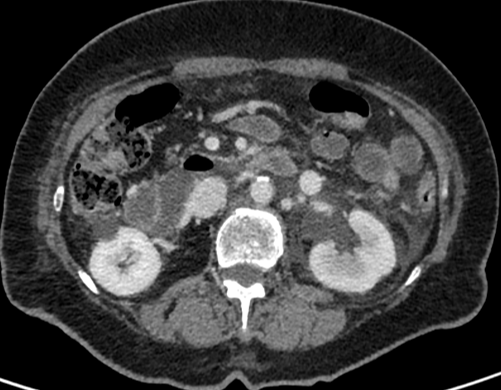
- Axial and coronal CECT images of the abdomen at the level of kidneys in venous phase.
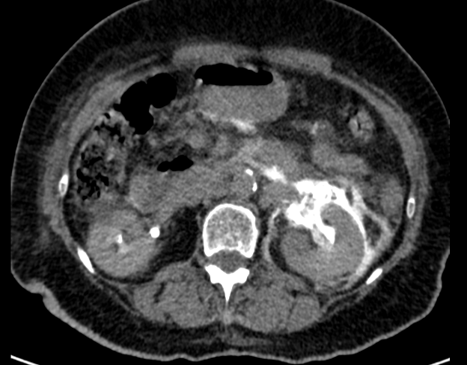
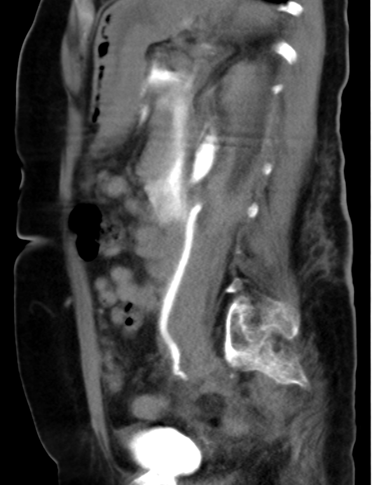
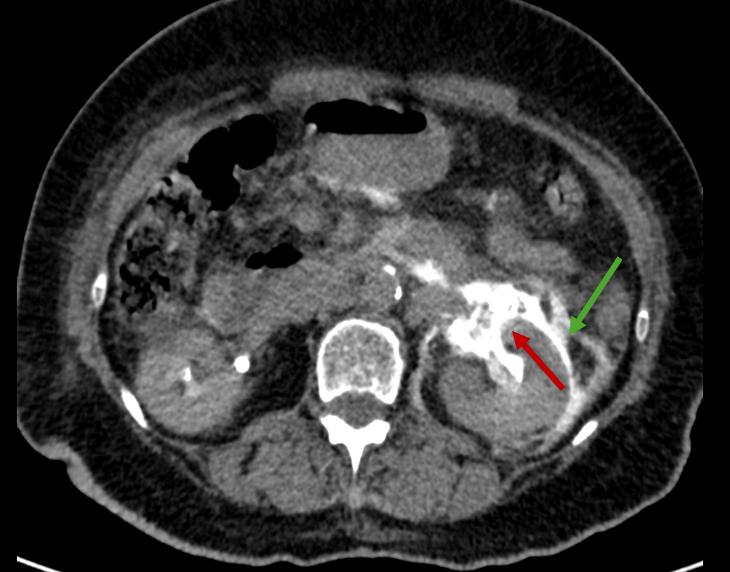
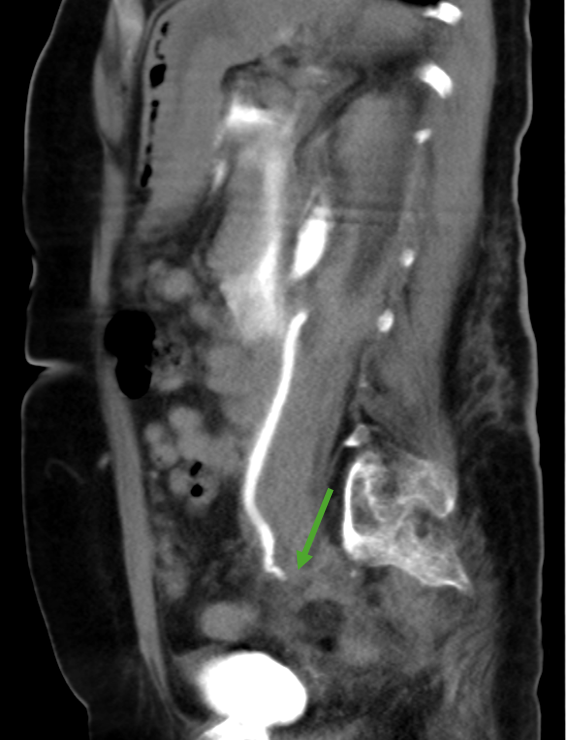
- Axial and sagittal CECT images of the abdomen in delayed phase.
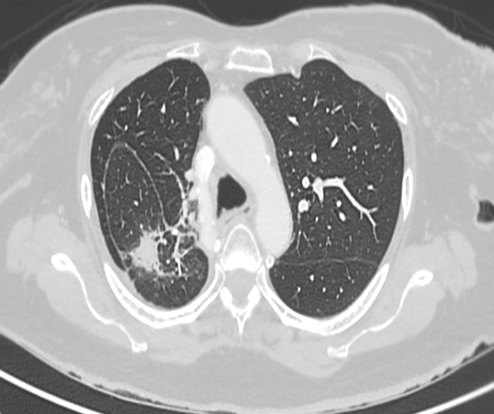
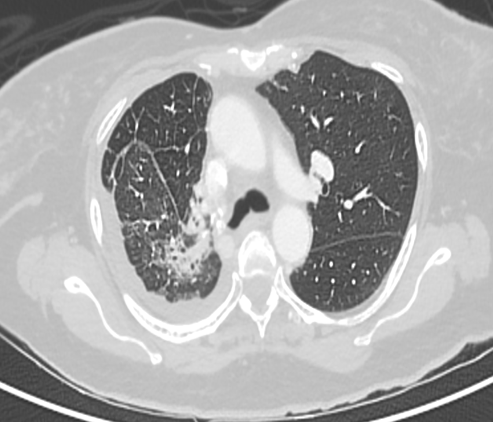


- Patchy consolidation with spiculated margins in the surgical bed. (red arrow) Surrounding lung parenchyma shows interstitial thickening and ground glass attenuation. (green arrow) Mild right pleural effusion.
- Left kidney appears hypo enhancing and shows perinephric fluid and fat stranding extending to the pararenal fascia. Mild ascites.
- On delayed imaging, the contrast is seen extravasating (red arrow) from the upper pole calyx (suggesting calyceal rupture) into the perirenal space and retroperitoneum (green arrow).
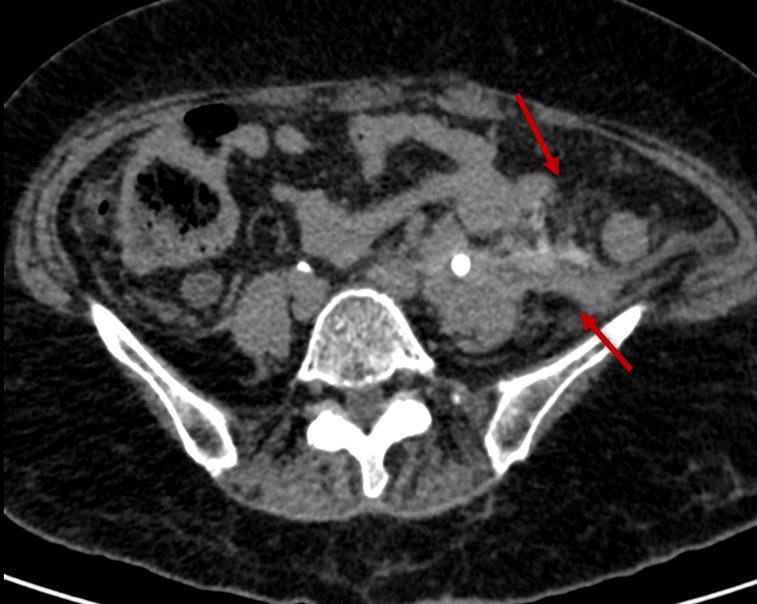
- Omental caking and peritoneal thickening seen in left lower quadrant. (red arrow)Short segment narrowing of the left distal ureter with abrupt cut off. (green arrow)



DIAGNOSIS :
- Distal ureteric obstruction causing upstream hydroureteronephrosis and calyceal rupture with urine extravasation. The obstruction likely reflects serosal / peritoneal disease.
MANAGMENT:
- Patient was managed with bilateral DJ stenting.
DISCUSSION :
INTRODUCTION:
- Hematogenous or lymphatic metastases from a distant primary neoplasm to the ureter are encountered infrequently.
- The rarity of their occurrence probably reflects the segmental distribution of the blood and lymphatic vessels in the ureter and periureteral sheath, resulting in the absence of continuous longitudinal networks. Secondarily, the lymph drainage of the ureter of the lower portion of the ureter is downward and counterdirectional to that of the pelvic organs.
- As the periureteral adventitial soft tissue is longitudinal, blood vessels are very well developed in this layer. This may be why hematogenous metastases occur more often in the periureteral tissue, and it is this periureteral tissue layer of the ureter that is usually first involved in metastases to the ureter.
- Lung cancer is the most common cause of cancer death for both genders. At the time of diagnosis, only 20% of all lung cancer patients will have local disease, while 55% will have distant metastatic disease.
- The brain is the most common site of metastases of lung cancer followed by the bones, liver, and adrenal glands. However, ureteral obstruction caused by metastases of lung cancer is extremely rare.
- Systemic chemotherapy and targeted therapy are usually used in patients with advanced lung cancer. However, patients with ureteral tumors usually present with ureteral hydronephrosis and expansion, which generally need surgical intervention.
- In patients of lung cancer, presence of hydronephrosis should alert the clinician to the possibility of metastasis and subsequent evaluation.
CLINICAL PROFILE:
- Most of the ureteric metastases are asymptomatic and incidentally diagnosed at autopsy.
- If symptoms occur, the patients usually present with pain in abdomen. In advanced cases, urinary symptoms or abdominal distension may occur.
- Frequently, symptoms of ureteric metastases are masked by severe debilitating disease due to the primary malignancy.
- Rarely, symptoms of ureteric obstruction may be the presenting feature of an underlying malignancy.
IMAGING, EVALUATION AND DIFFERENTIAL DIAGNOSIS:
- Radiographic findings of extrinsic ureteral obstruction due to metastatic diseases depend on the pattern of the tumoral spread: hematogenous submucosal/mucosal metastasis, hematogenous adventitia metastases spreading along periureteral vessels, scirrhous metastatic spread along periureteral vessels, or metastatic spread into lymph nodes with perinodal desmoplastic reaction.
- The detection of asymmetric wall enhancement, wall thickening, and urinary obstruction (hydronephrosis, hydroureter, adjacent inflammatory changes, urinary leak, urinoma formation, ascites) are the expected imaging findings.
- From an imaging standpoint, the differentiation of ureteral metastasis from primary urothelial tumors might be difficult or even impossible. Primary uroepithelial tumors of the ureter typically involve a long segment and demonstrate multifocality, whereas secondary tumors usually affect a relatively short segment. Clinical history may also help differential diagnosis as some tumors are more prone to uroepithelial metastasis than others.
- Strictures after stone passage, distal ureteral stenosis due to tuberculosis, amyloidosis, and endometriosis should be considered in the differential diagnosis
- Endoscopic evaluation of the ureters with histopathologic evaluation may be required in most of the cases.
TREATMENT AND CONCLUSION:
- The patients are usually managed with excision of diseased segment and DJ stenting.
- Nephrostomy or, in some cases, ureteric reimplantation is indicated when ureteral catheterization is not possible. Nephrectomy is only rarely required.
- Whenever ureteral metastasis is suspected, early and aggressive workup followed by appropriate treatment may preserve renal function and increase the survival rate.
- Ureteral metastases are very rare but must be kept in the differential diagnosis when a patient who has malignant disease has evidence of ureteral obstruction on radiographic studies. The presence of ureteral metastases indicates advanced disease and the prognosis is bleak.
REFERENCES:
- Mamlouk MD, Vansonnenberg E, Shankar S, Silverman SG. Omental cakes: unusual aetiologies and CT appearances. Insights Imaging. 2011 Aug;2(4):399-408. PMCID: PMC3259316.
- Kodama K, Imao T, Komatsu K. Metastatic ureteral involvement of non-small cell lung cancer. Case Rep Med. 2011;2011:394326. PMCID: PMC3085393.
- Karaosmanoglu AD, Onur MR, Karcaaltincaba M, Akata D, Ozmen MN. Secondary Tumors of the Urinary System: An Imaging Conundrum. Korean J Radiol. 2018 Jul-Aug;19(4):742-751. PMCID: PMC6005933.
Dr Madhukumar
Senior Consultant Radiologist,
MHRG, Manipal Hospital, Yeshwanthpur.
Dr Kanupriya Grover
Cross Sectional Imaging Fellow,
MHRG, Manipal Hospital, Yeshwanthpur.

