
70-year-old lady presented with severe acute abdominal pain and vomiting
A 70-year-old lady presented with severe acute abdominal pain and vomiting.
Findings:-
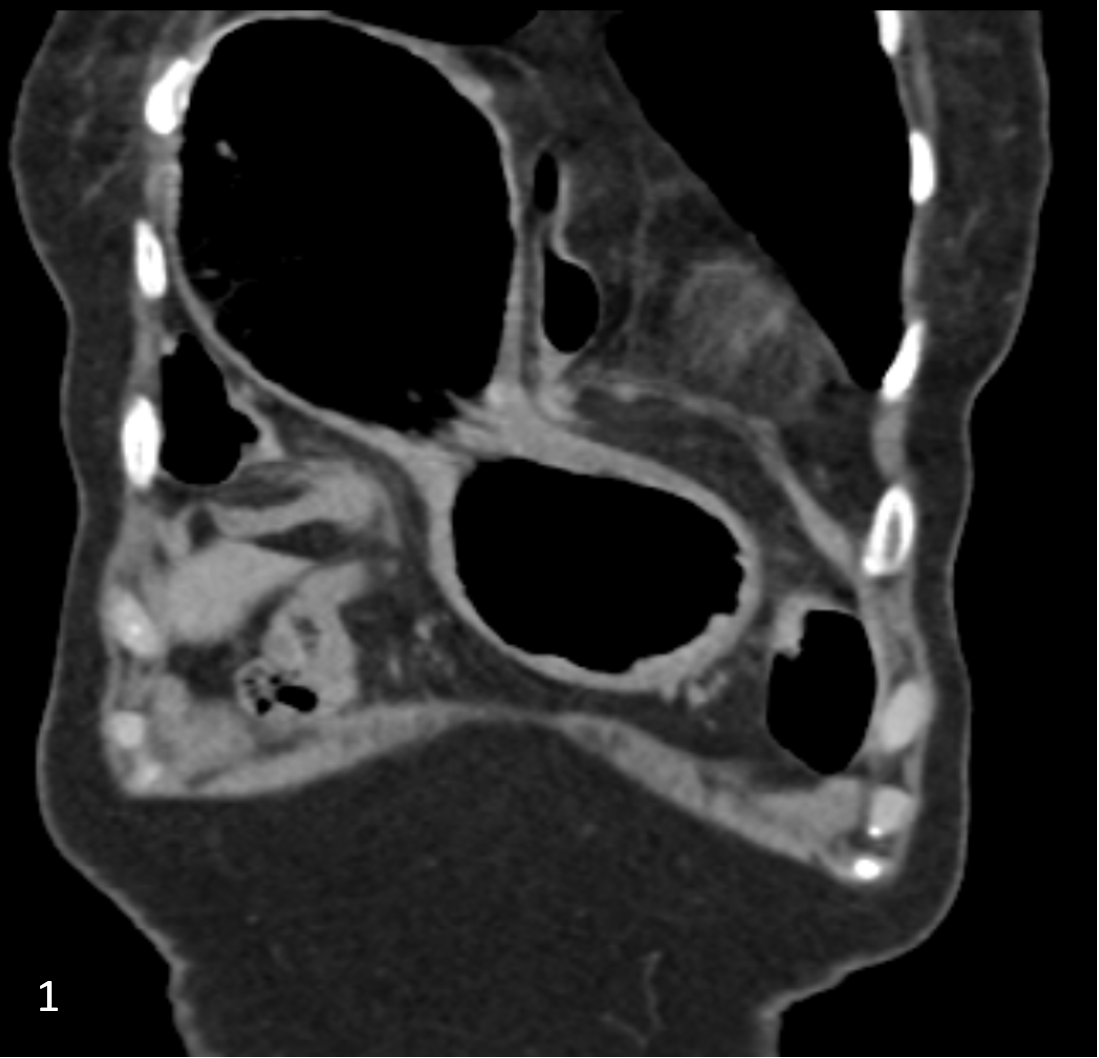
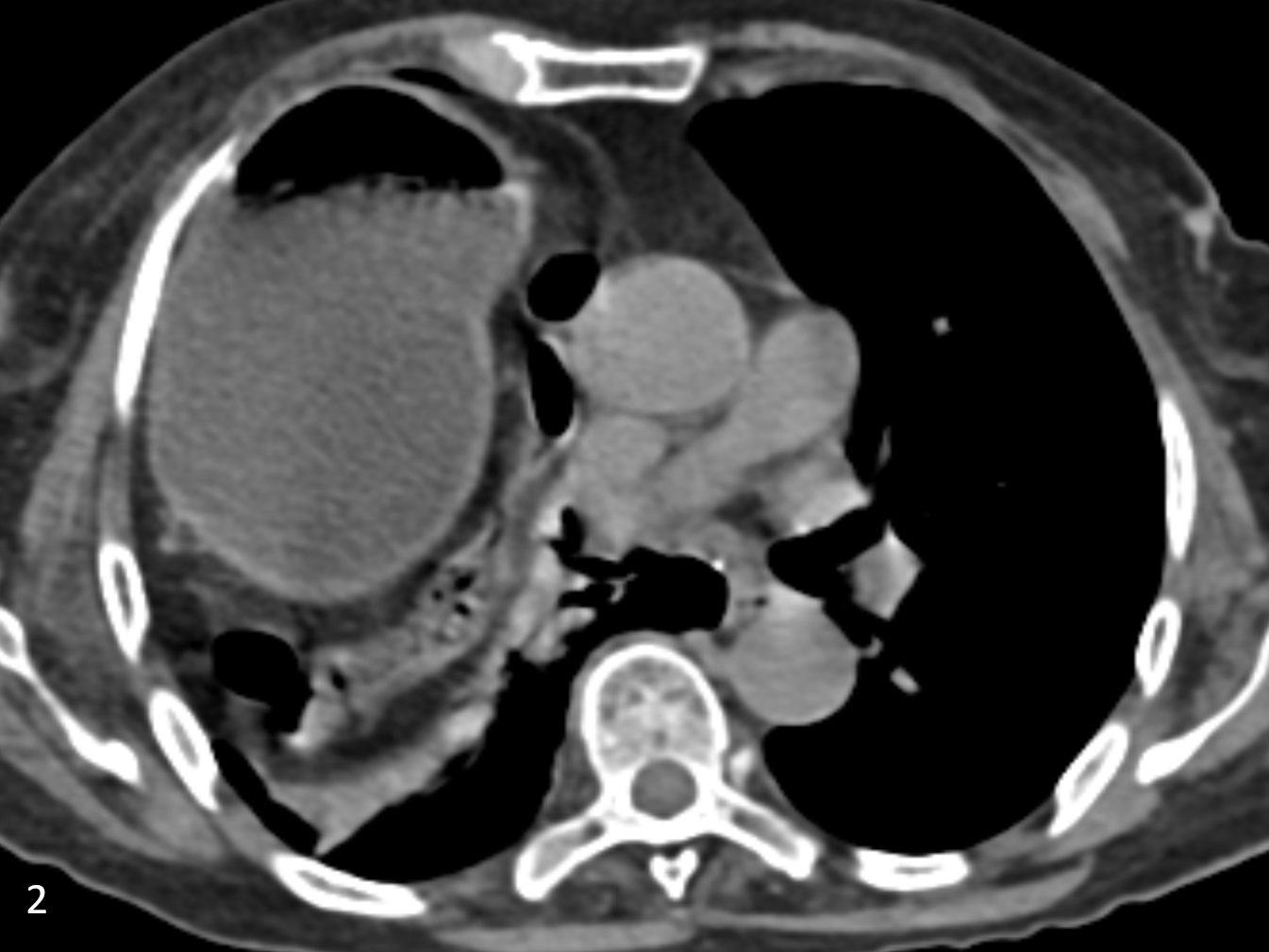
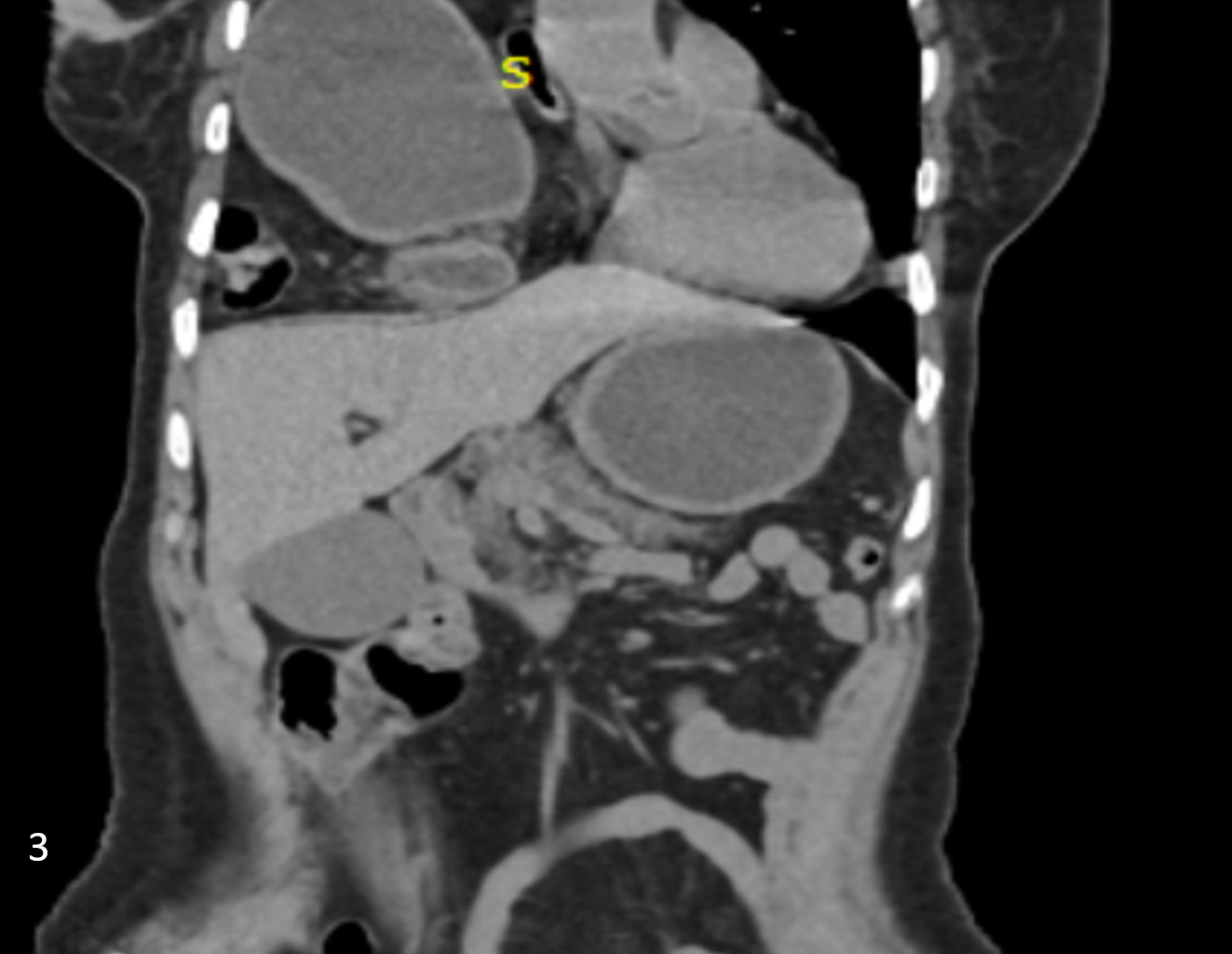
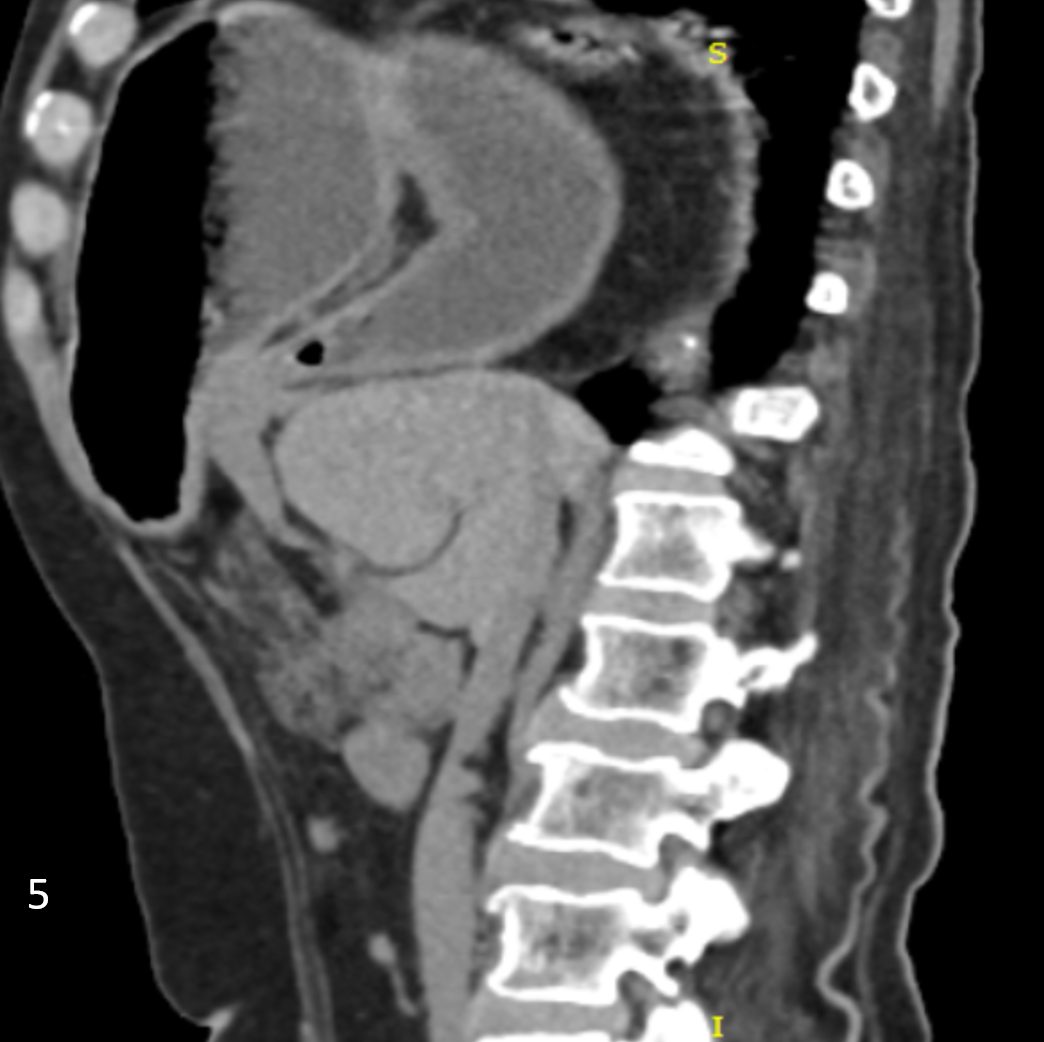
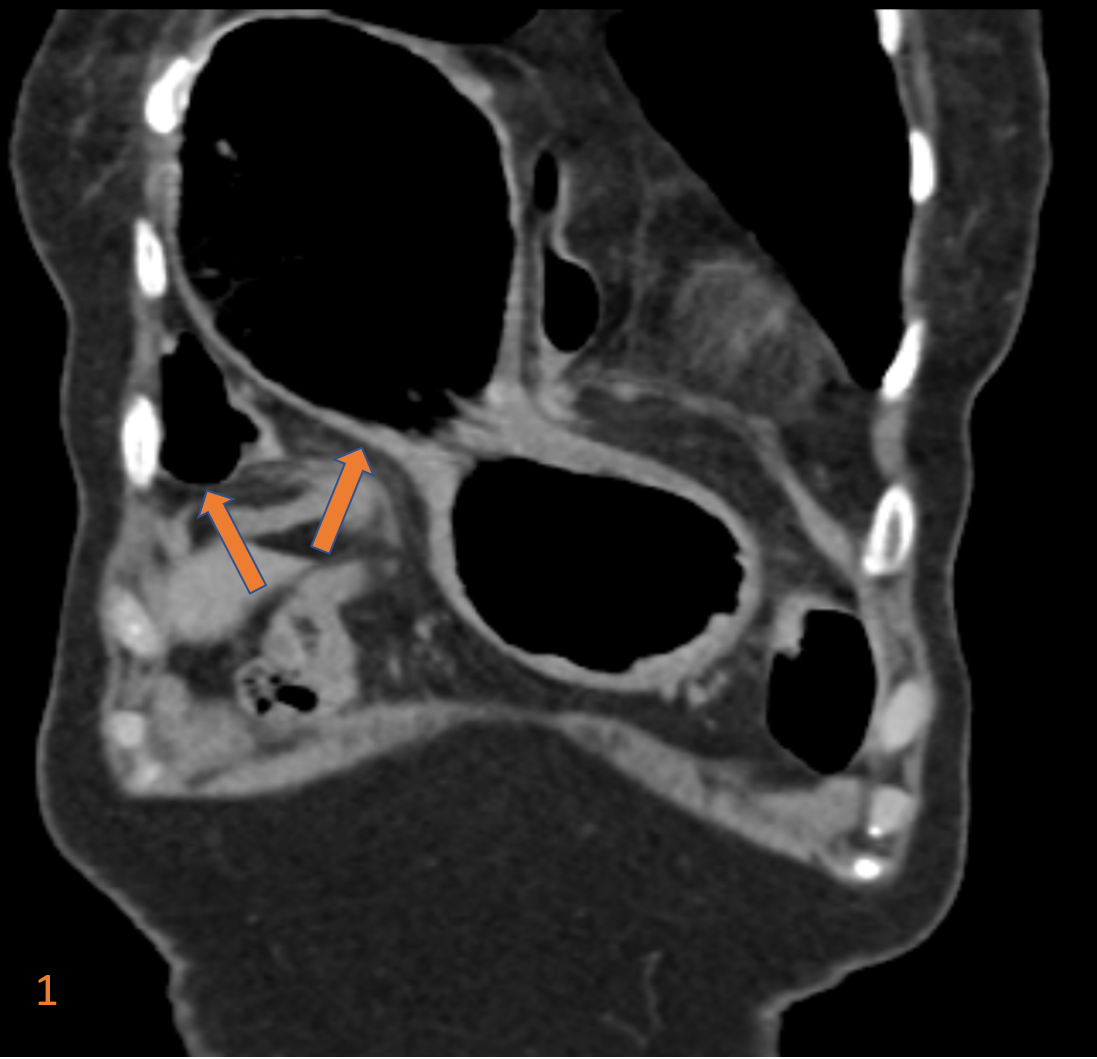
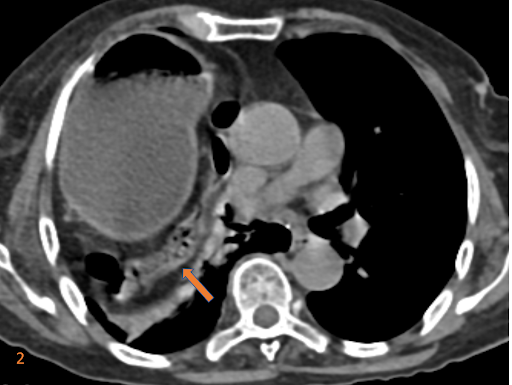
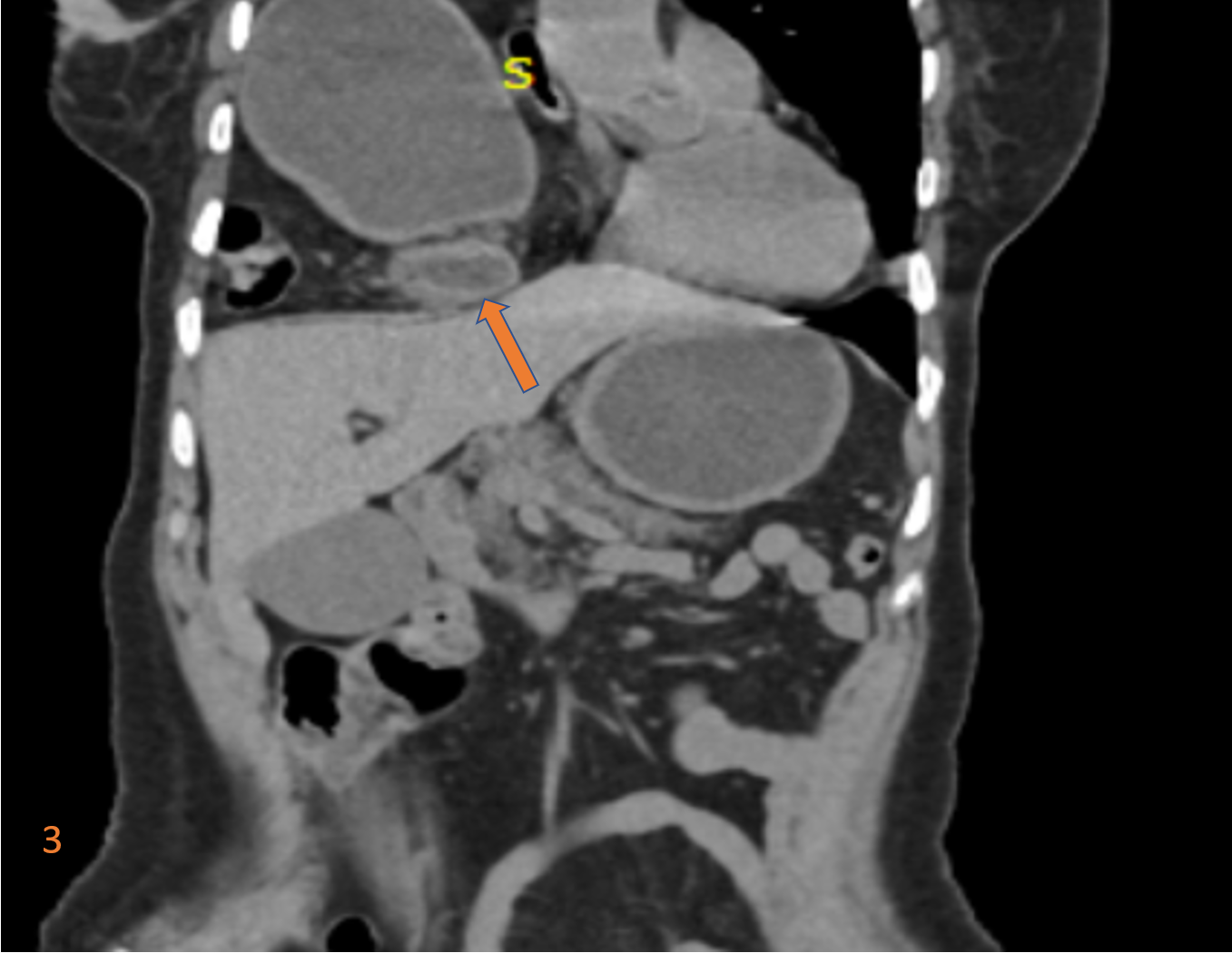
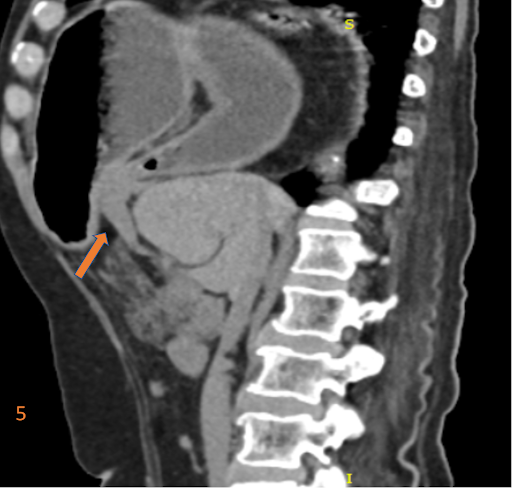
- There is herniation of the body, antrum, pylorus of stomach, 1st part of duodenum, transverse colon, gastrocolic ligament and transverse mesocolon through the foramen of Morgagni on the right into the right hemithorax. (Fig. 1-3)
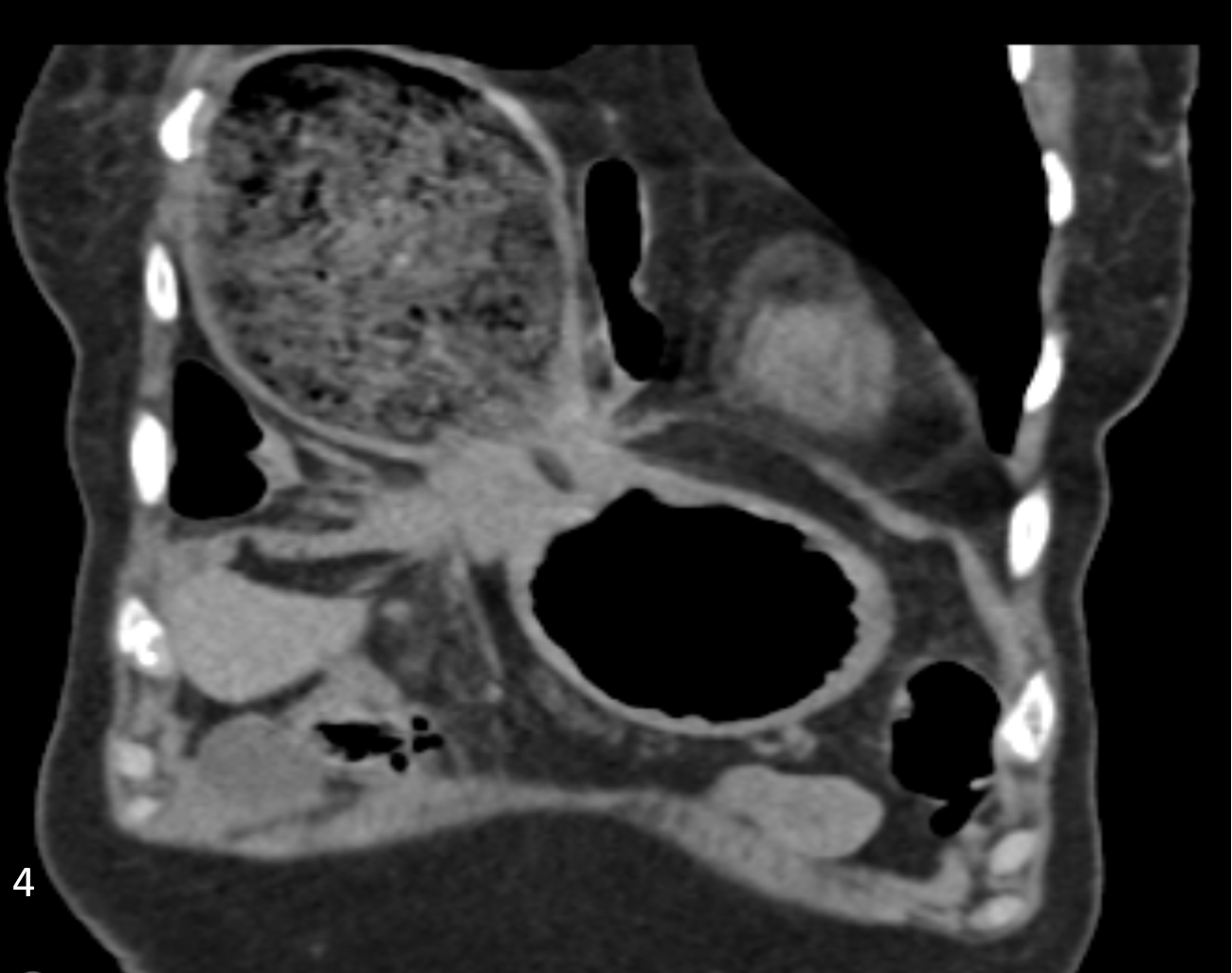
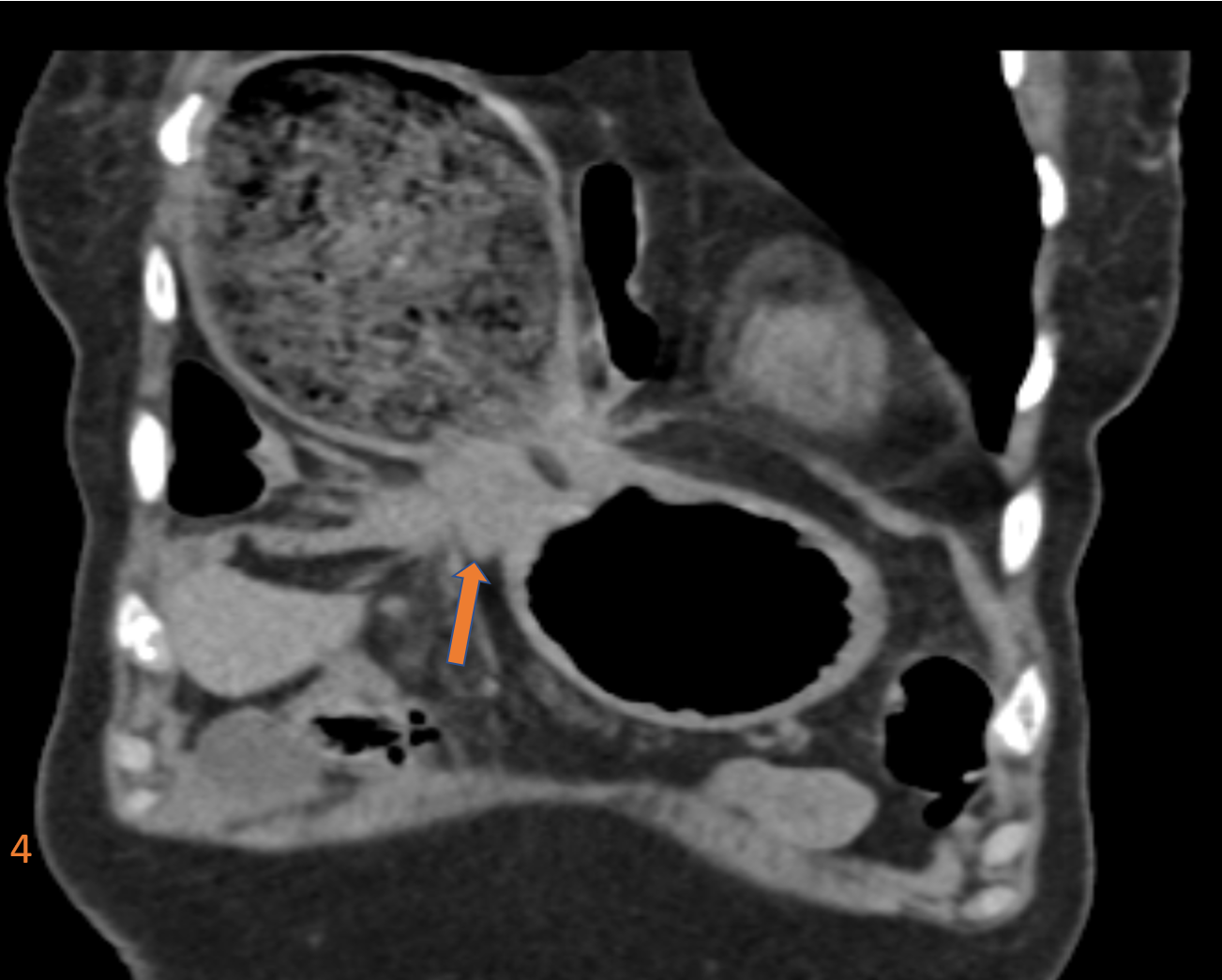
- The pylorus / first part of duodenum is located at the mouth of the hernial defect with compression and mild wall edema (Fig.4) casuing outlet obstruction.
- There is no evidence of volvulus.
- Antero-medial defect in right dome of diaphragm (Fig. 5)
DIAGNOSIS:
Morgagni Hernia with gastric herniation and gastric outlet obstruction.
DISCUSSION:
- Morgagni hernias are one of the congenital diaphragmatic hernias, and are characterized by herniation of abdominal content through the foramen of Morgagni.
- Conditions such as pregnancy, trauma, chronic cough, obesity and constipation, all of which may increase intraabdominal pressure predisposes the condition
- Morgagni hernias are:
- Anteromedial parasternal defect (Space of Larrey)
- Due to a maldevelopment of septum transversum
- known to occur in overweight, middle-aged, women
- Right > left (heart protects the left side)
- Usually not large and usually, unilateral
- Associated with
- Pericardial defects
- Omental fat in pericardial space
- Imaging differentials include:
-
-
- Cardio-phrenic angle lesions: the main differential diagnosis for Morgagni hernia is a cardiophrenic fat pad.
- Focal diaphragmatic eventration: an abnormal elevation of one leaf of an intact diaphragm as a result of paralysis, aplasia, or atrophy of varying degrees of muscle fibers
- Diaphragmatic rupture: history of trauma and other supportive signs of chest and/or abdominal trauma would be apparent. This is most commonly seen posterior and postero-laterally (Fig. 7)
-

-
-
- Gastric Volvulus:The stomach is twisted over its axial plane (short axis) along the mesenteric attachment with a replaced position of the gastroesophageal and the pyloroduodenal junction, with the latter being in superior level. (Fig. 8 and 9)
-


REFERENCES:
- Kumar A, Bhandari RS. Morgagni hernia presenting as gastric outlet obstruction in an elderly male. J Surg Case Rep. 2016;2016(7):rjw126. Published 2016 Jul 18. doi:10.1093/jscr/rjw126
- El-shark away A, Higashi Y, Lobo D. Education, and imaging. Gastrointestinal: foramen of Morgagni hernia in an adult. J. Gastroenterol. Hepatol. 2012;27 (3): 616. doi:10.1111/j.1440-1746.2012.07055.x –
- Aghajanzadeh M, Khadem S, Khajeh jahromi S et-al. Clinical presentation and operative repair of Morgagni hernia. 2012;doi:10.1093/icvts/ivs203 –
Case contributed by:
Dr. Suvarna Kote,
Radiology resident
Columbia Asia Radiology Group.
Dr. Sunita Gopalan
DMRD, FRCR
Senior Consultant Radiologist
Columbia Asia Radiology Group

