
63 year old male patient presented with swelling in the perianal region, associated with bleeding from rectum for 1 year.
- 63 year old male patient presented with swelling in the perianal region, associated with bleeding from rectum for 1 year.
- History of weight loss.
- Past history of treated fistula in ano.
- On examination: Fungating exophytic growth in the sacral region and perianal region.
- MRI fistulogram and a correlative CT was performed.
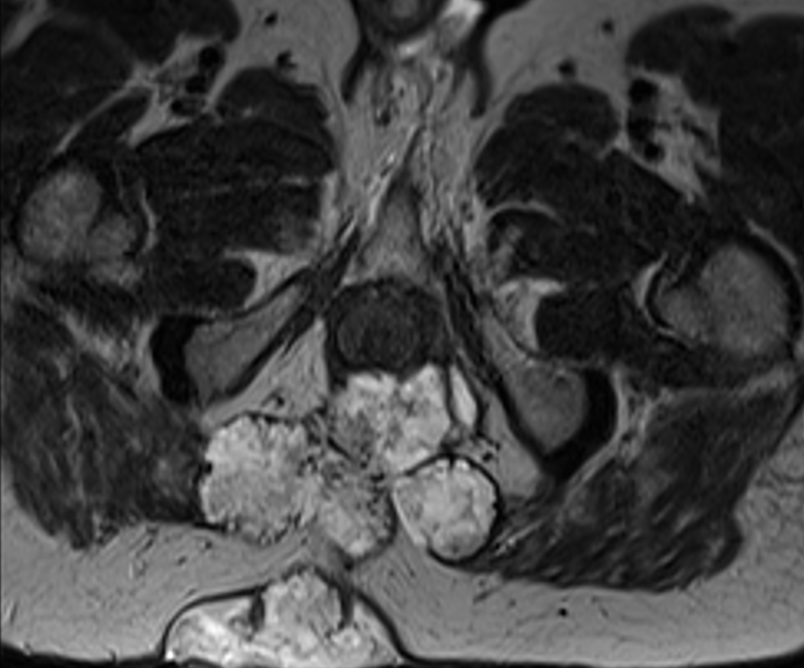


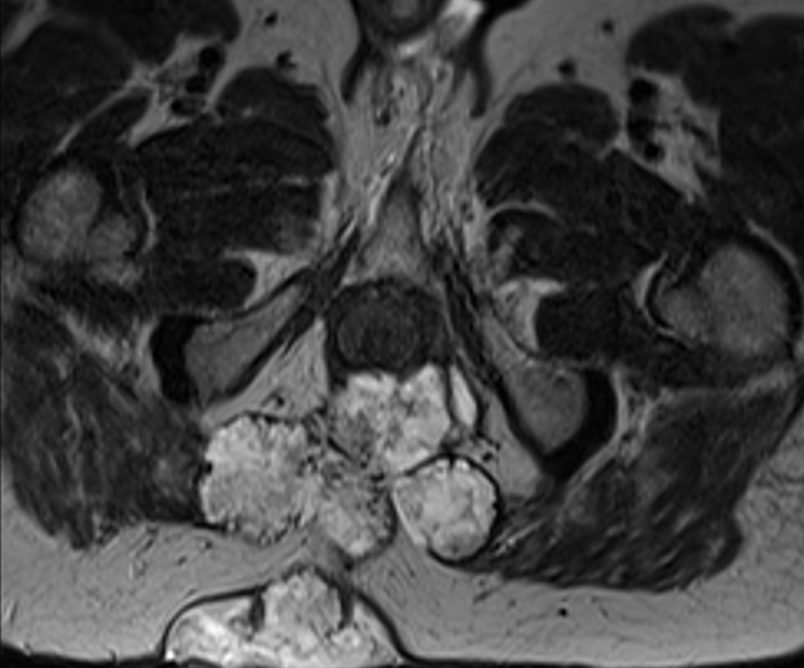
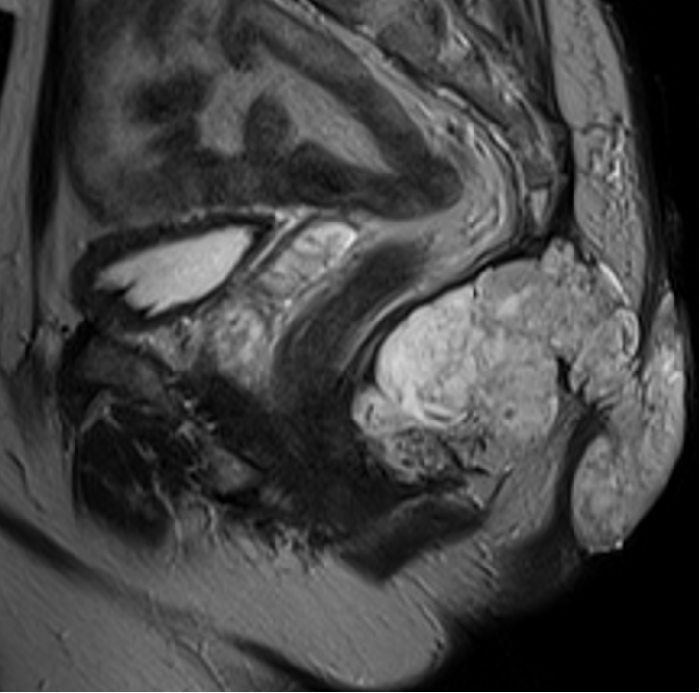
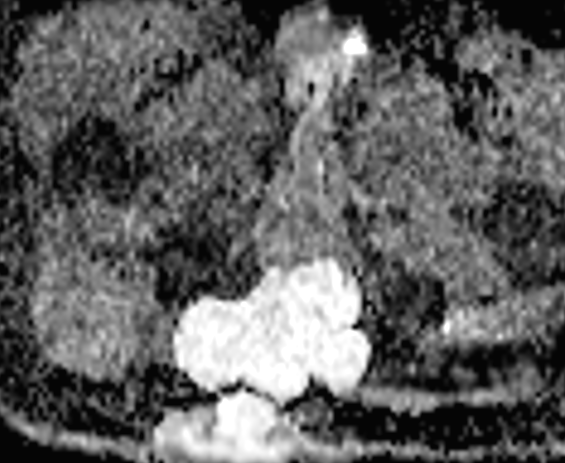
- A. Ill-defined T2 heterogeneously, hyperintense lesion with lobulated margins, in the infracoccygeal region, extending into the bilateral ischiorectal fossa and posteriorly into the subcutaneous plane as an exophytic growth. Anteriorly, the lesion is abutting the puborectalis, with loss of fat planes in the inferior aspect.
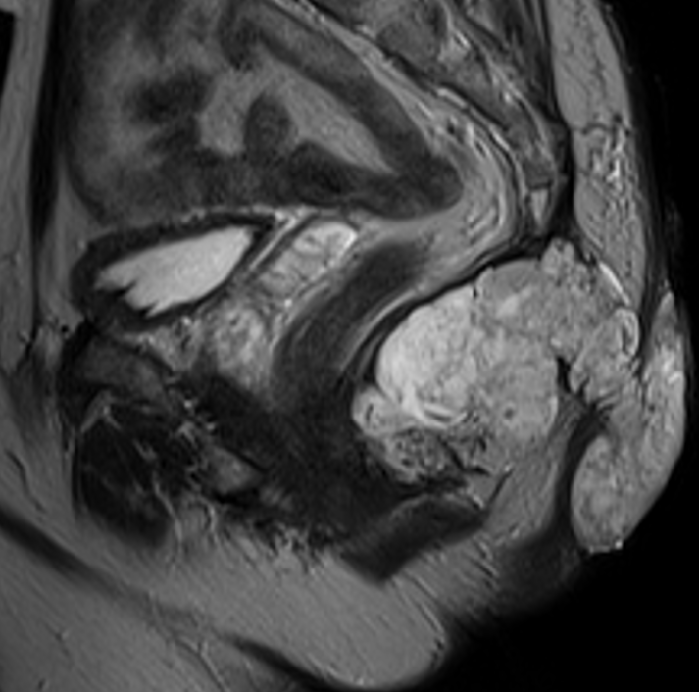
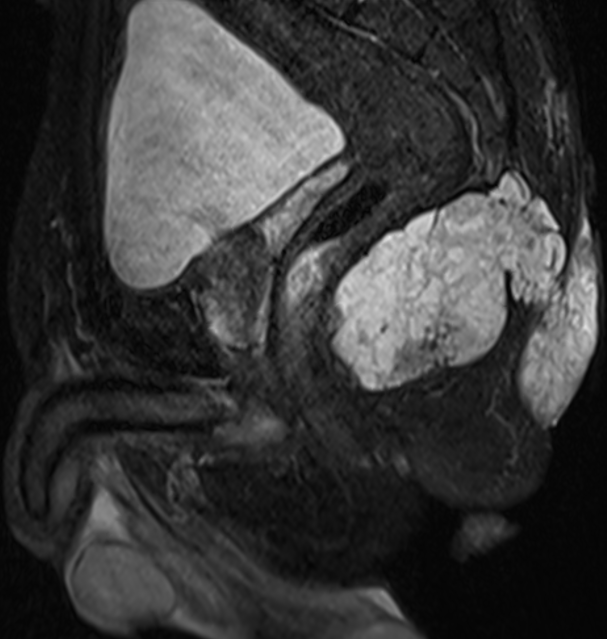
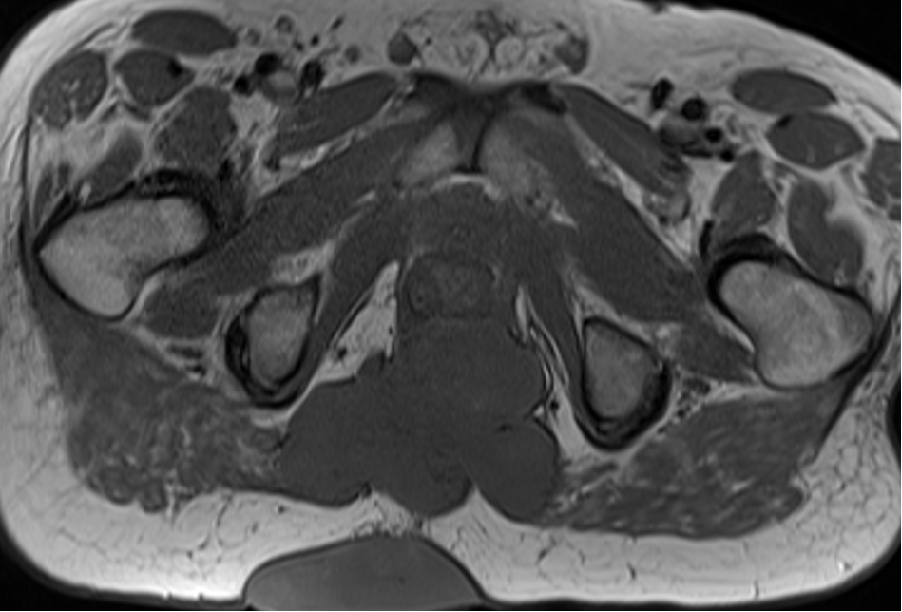
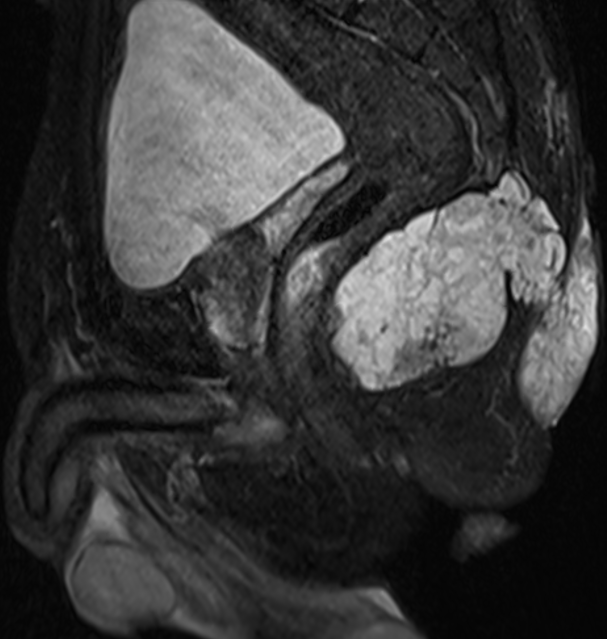
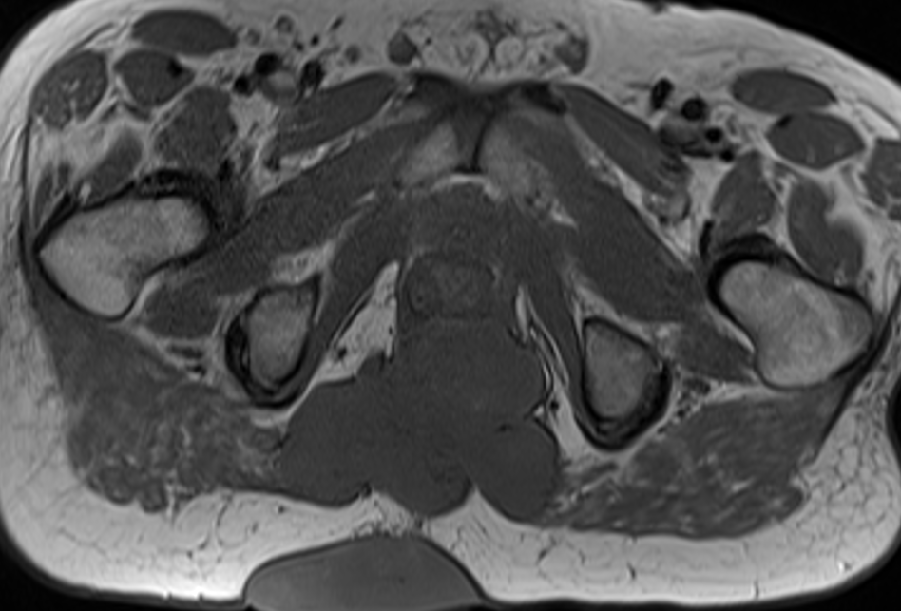
- B. The lesion is isointense on T1 and demonstrates STIR hyperintensity.
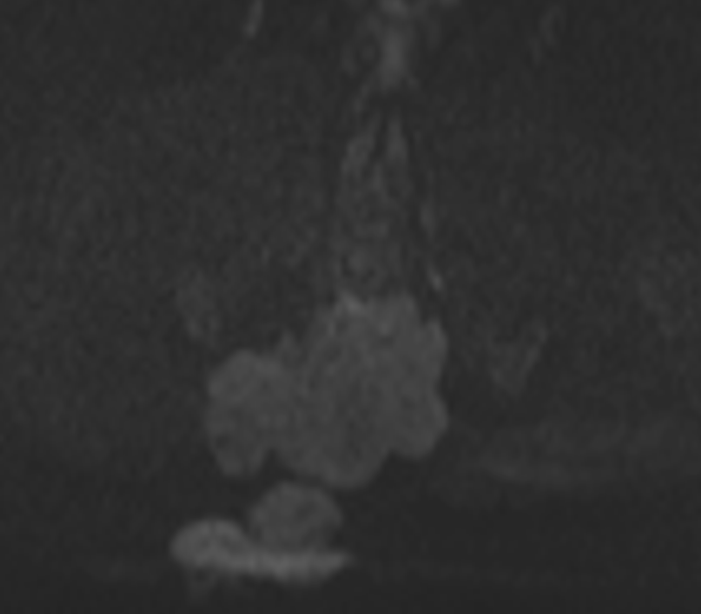
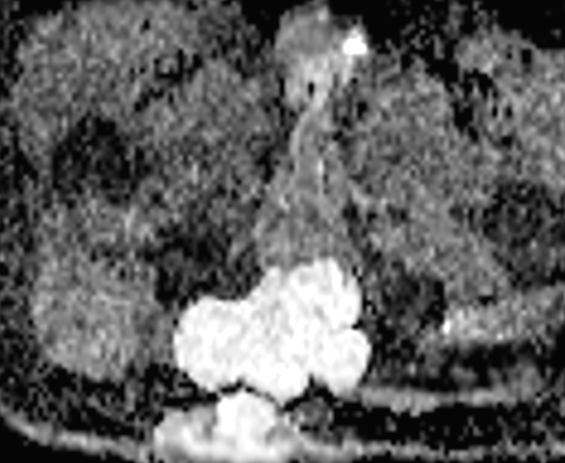
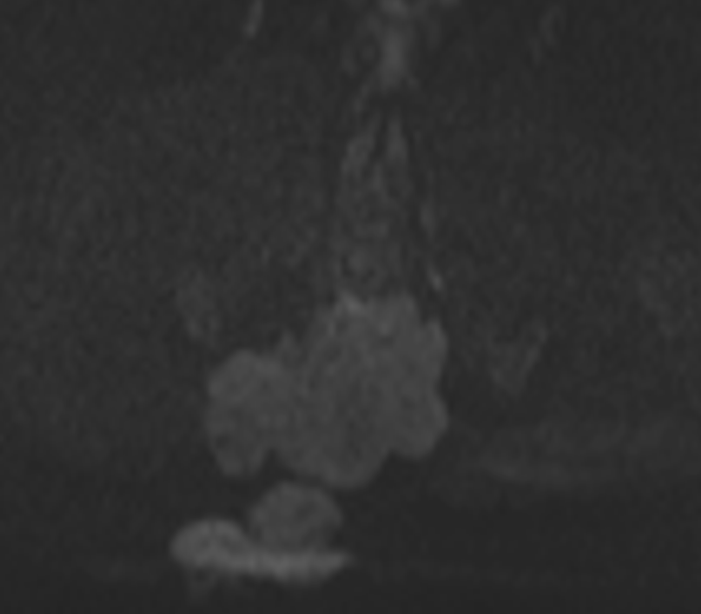
- C. The lesion does not demonstrate restricted diffusion.
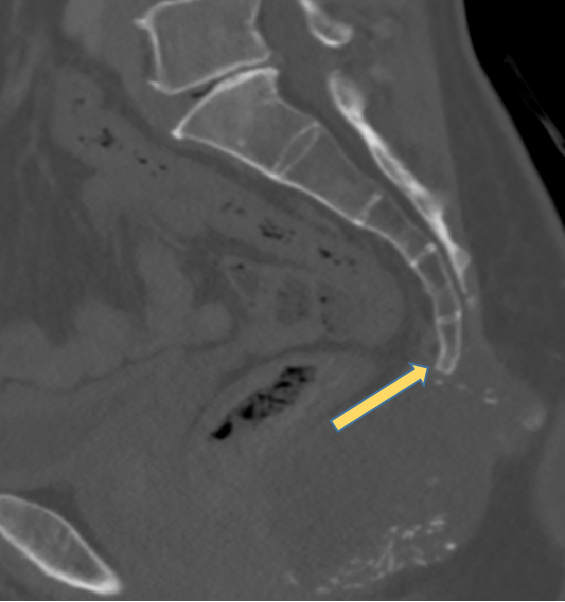
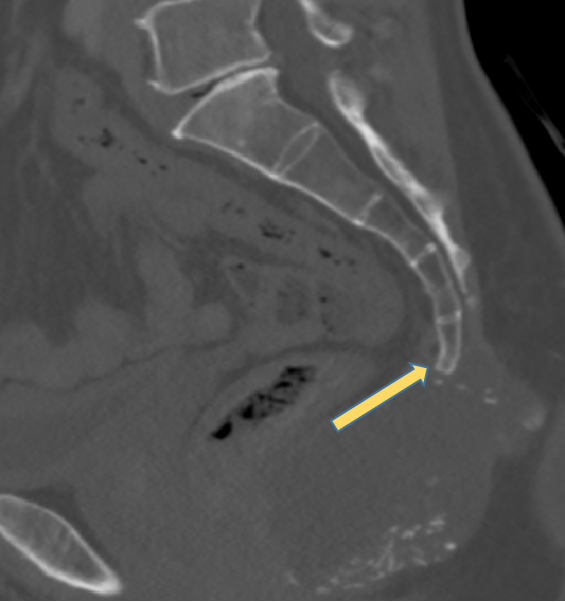
- D. Arc like calcification along the periphery of the lesion. Lesion is abutting the tip of the coccyx with destruction of the tip of the coccyx.


DIAGNOSIS
- Imaging diagnois: Aggressive coccygeal bone tumor (Probably chondrosarcoma).DD : Mucinous adenocarcinoma
- HPE: Mucinous adenocarcinoma – Grade II [Moderately Differentiated].
- Blood investigations showed raised CEA (24.3).
- Underwent sigmoidoscopy - Rectal polypoidal lesion- Goblet cell rich traditional serrated adenoma with Foci of high grade dysplasia.
- Started on chemotherapy with FOLFOX
DISCUSSION
- Mucinous adenocarcinoma arising from chronic perianal fistula is an uncommon neoplasm.
- It has been suggested that malignant degeneration of a longstanding perianal fistula is often associated with mucosal regeneration.
- Some authors believe malignant cells settle in the fistulous granulation tissue arising from proximal gastrointestinal neoplasms.
- Although metastases to inguinal lymph nodes may be present in advanced cases, distant metastases are uncommon.
- However, they are locally aggressive and entail a high probability of local recurrence.
- Early diagnosis of perianal adenocarcinoma is difficult as the tumor does not pierce the rectal mucosa and its course is usually indolent.
- Presence of T2-hyperintense mucin within a tumor at pretherapy MRI - independent biomarker for poor prognosis and poor therapy response
- Due to overall decreased cellularity, they show less enhancement and diffusion restriction compared with nonmucinous tumors.
REFERENCES
- Díaz-Vico T, Fernández-Martínez D, García-Gutiérrez C, Suárez-Sánchez A, Cifrián-Canales I, Mendoza-Pacas GE, Sánchez-Farpón H, Truán-Alonso N. Mucinous adenocarcinoma arising from chronic perianal fistula—A multidisciplinary approach. Journal of Gastrointestinal Oncology. 2019 Jun;10(3):589.
- Hama Y, Makita K, Yamana T, Dodanuki K. Mucinous adenocarcinoma arising from fistula in ano: MRI findings. American Journal of Roentgenology. 2006 Aug;187(2):517-21.
Dr Madhukumar
Senior Consultant Radiologist
Manipal Hospital, Yeshwanthpur
Dr Rashmi Jayakar Poojary
Junior Radiology Resident
Manipal Hospital, Yeshwanthpur

