
54 year old lady, presented with severe abdominal pain and obstipation for 4 days
- 54 year old lady, presented with severe abdominal pain and obstipation for 4 days.
- No history of fever or vomiting.
- Past surgical history – Underwent LSCS 3 times.
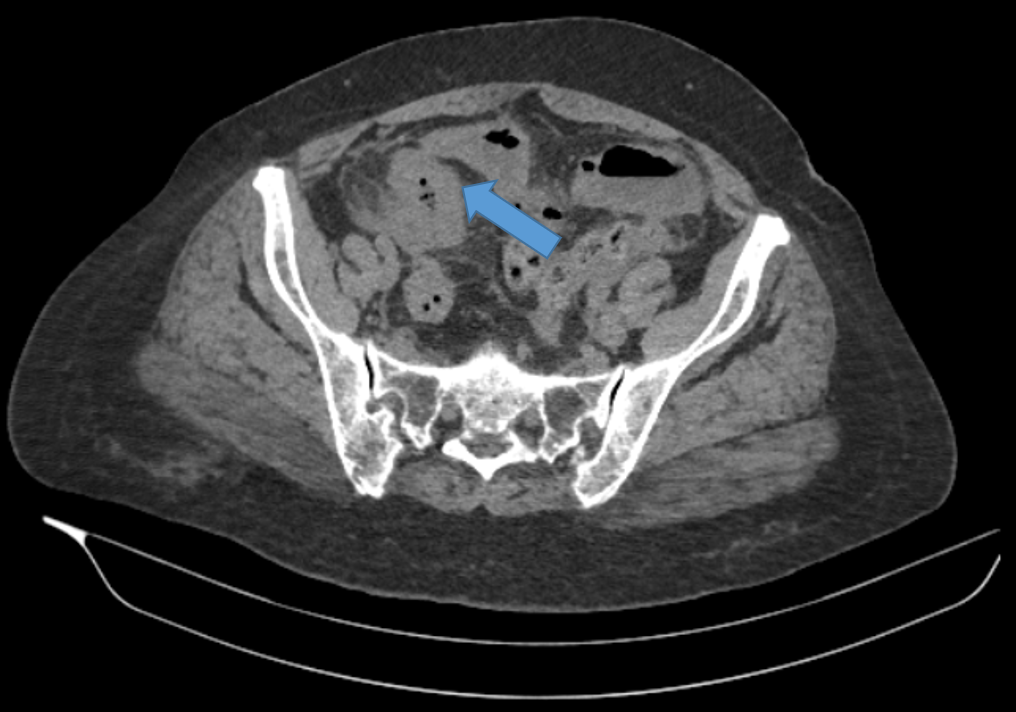
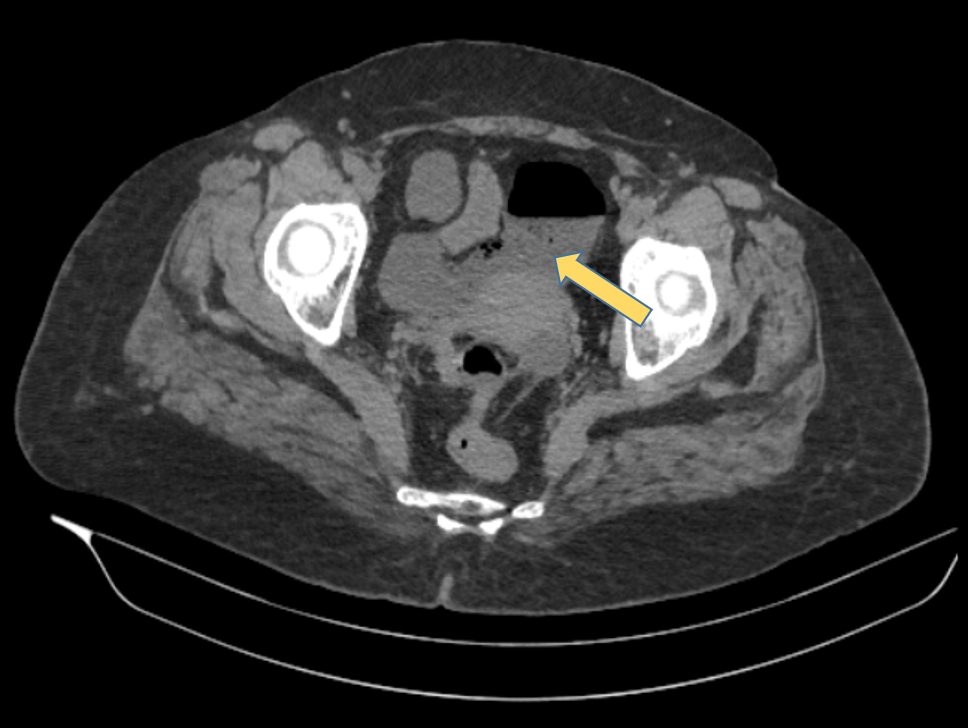
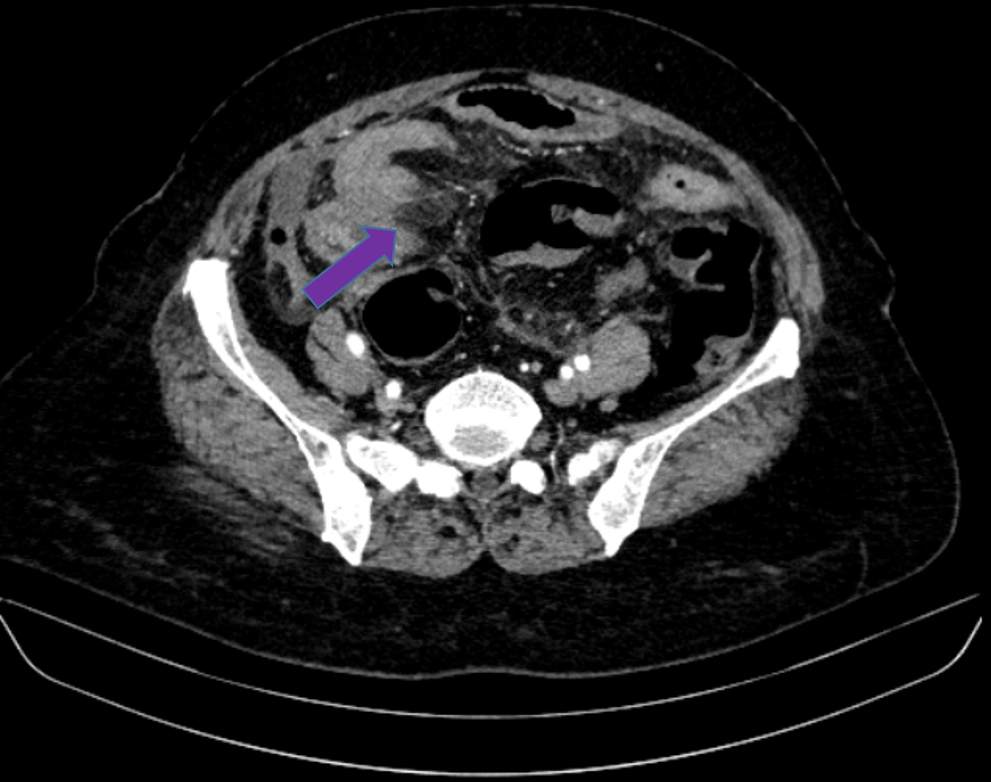
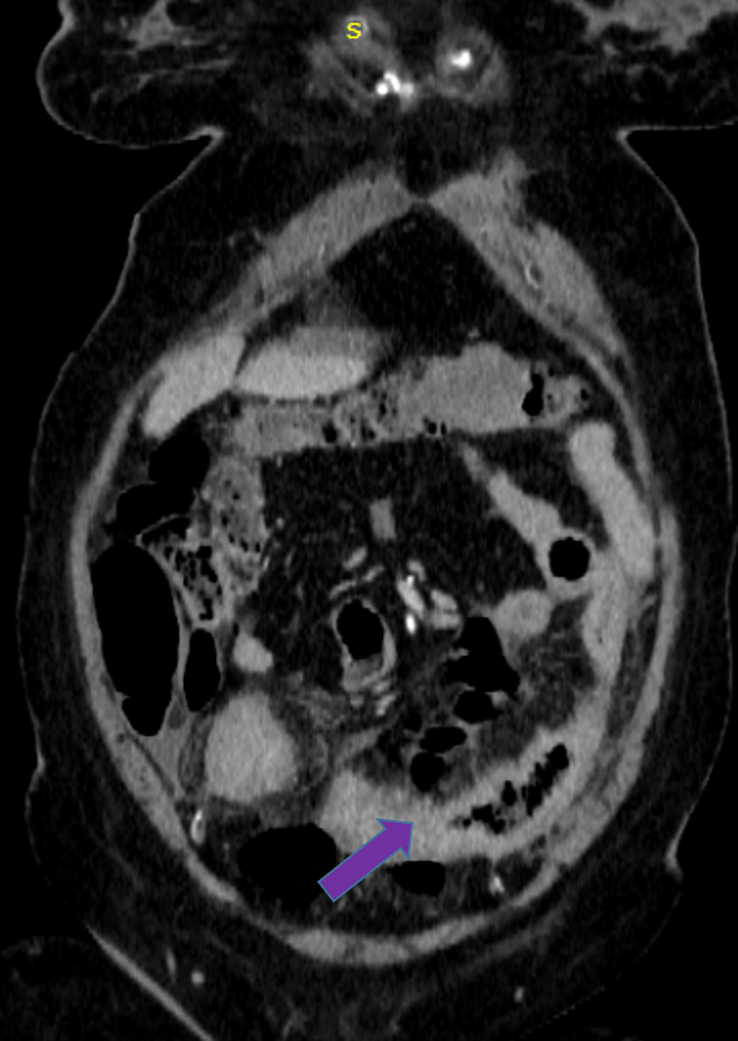
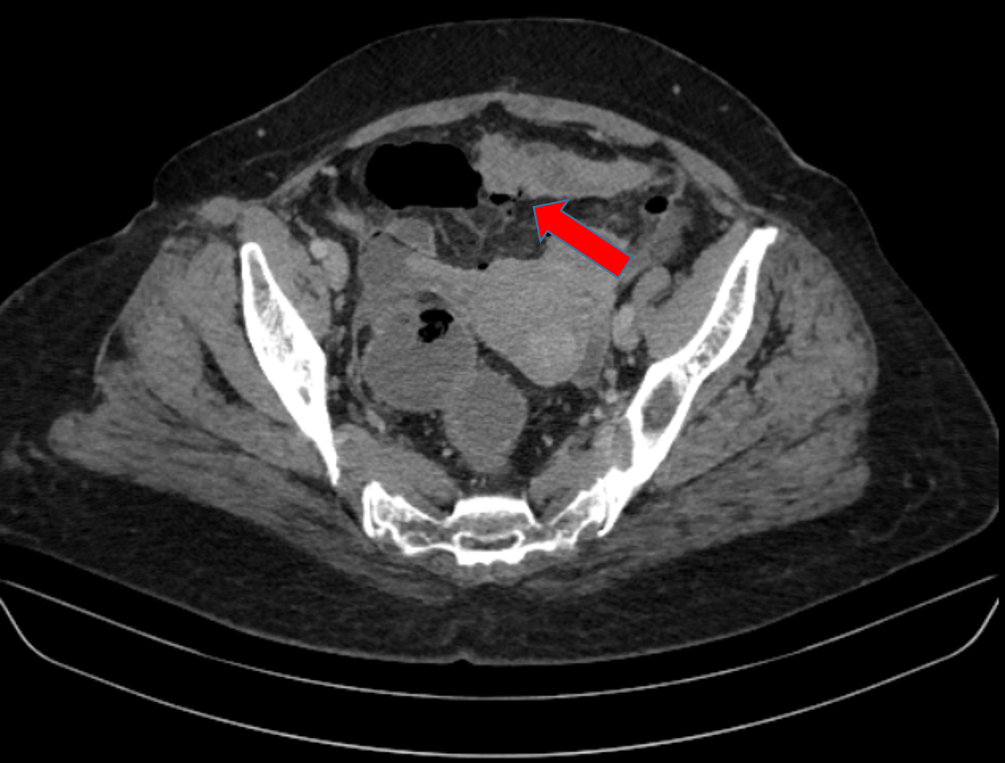
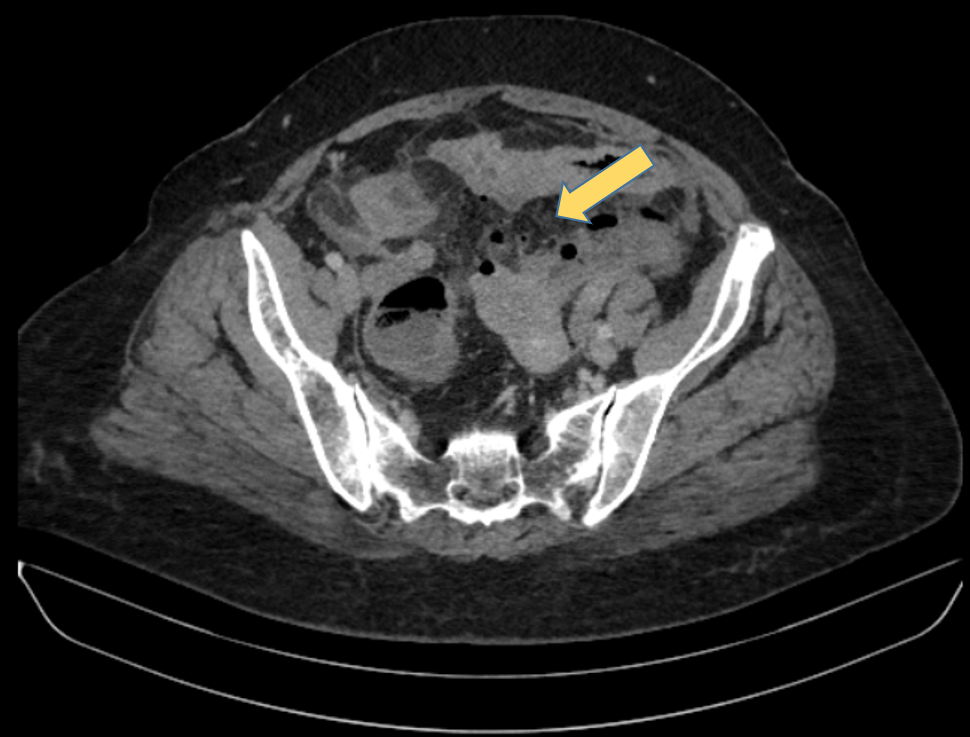
FINDINGS
DIAGNOSIS
- Crohn’s disease with ileal perforation and peritonitis.
DISCUSSION:
- Crohn disease is an idiopathic inflammatory bowel disease characterized by discontinuous gastrointestinal tract inflammation.
- The terminal ileum and proximal colon are most often affected.
- Patients typically present with chronic diarrhea and recurrent abdominal pain, although occasionally the presentation is with a complication or an extraintestinal manifestation.
- CT is the first imaging assessment for patients in the setting of an acute abdomen or for reassessment of complications in patients with known Crohn disease.
Common CT Imaging features include:
- Mural hyperenhancement
- Fat halo sign: submucosal fat deposition
- Bowel wall thickening which is most frequently seen in the terminal ileum.
- Comb sign: engorgement of the vasa recta
- Perienteric fat stranding.
- Affected bowel loops separated by focal/regionally increased fat (fibrofatty proliferation; creeping fat)
- Strictures and fistulae with upstream dilatation.
- Mesenteric/intra-abdominal abscess or phlegmon formation
Complications include:
- Strictures.
- Adhesions and bowel obstructions.
- Fistulae.
- Perianal fistula.
- Perianal abscess.
- Bowel perforation with free peritoneal air is a rare complication of Crohn’s disease.
- It is seen to occur in 1–3% of Crohn’s disease patients as a first manifestation or, in the course of the disease.
- Early diagnosis of bowel perforation is important and determines the survival rate.
- Only 20% of patients with Crohn’s disease and intestinal perforation have pneumoperitoneum on X-ray of the abdomen and/or on erect chest X-ray. Thus CT plays a pivotal role in accurate diagnosis of both Crohn’s disease and also in determining the site of intestinal perforation.
- Laparotomy and bowel resection should be considered if the perforation place is identified. However, in the absence of a clear site of perforation and without enteric contamination, a conservative surgical approach should be considered.
REFERENCES
- Furukawa A, Saotome T, Yamasaki M et al. Cross-Sectional Imaging in Crohn Disease. Radiographics. 2004;24(3):689-702. doi:10.1148/rg.243035120 – Pubmed
- Gore R, Balthazar E, Ghahremani G, Miller F. CT Features of Ulcerative Colitis and Crohn’s Disease. AJR Am J Roentgenol. 1996;167(1):3-15. doi:10.2214/ajr.167.1.8659415 – Pubmed.
- R.F. Leal et al. Free peritoneal perforation in a patient with Crohn’s disease – Report of a case. International Journal of Surgery Case Reports 4 (2013) 322–324.
Dr. Vishwanath Joshi
Consultant Radiologist.
Manipal Hospital Radiology Group (MHRG)
Manipal Hospital, Bengaluru.
Dr Rashmi Jayakar Poojary
Radiology resident
Manipal Hospital, Yeshwanthpur, Bengaluru.
