
52 year old male with post prandial distress and bloating followed by abdomen pain and vomiting
52 year old male with
- post prandial distress
- bloating
- followed by abdomen pain and vomiting
OGD - distal oesophageal corckscrew morphology and diverticulum , Gastric erosions
FINDINGS:
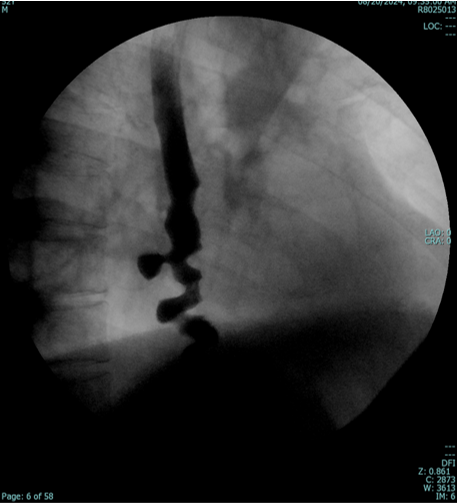
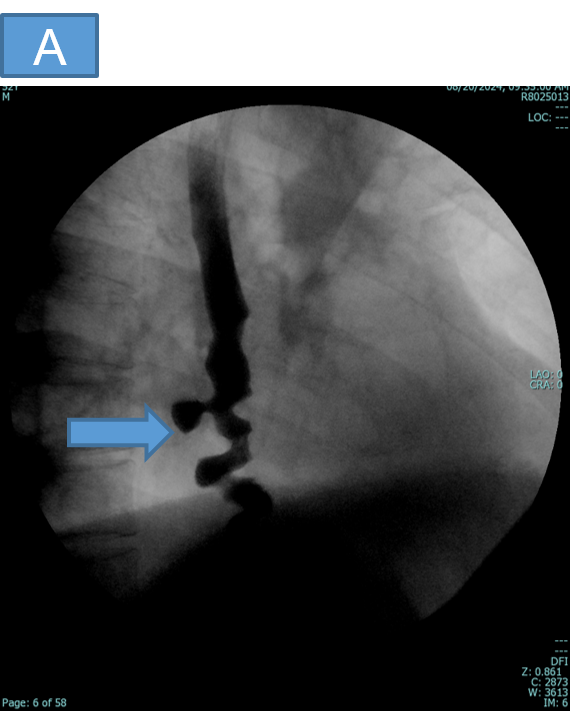
- A : BARIUM SWALLOW
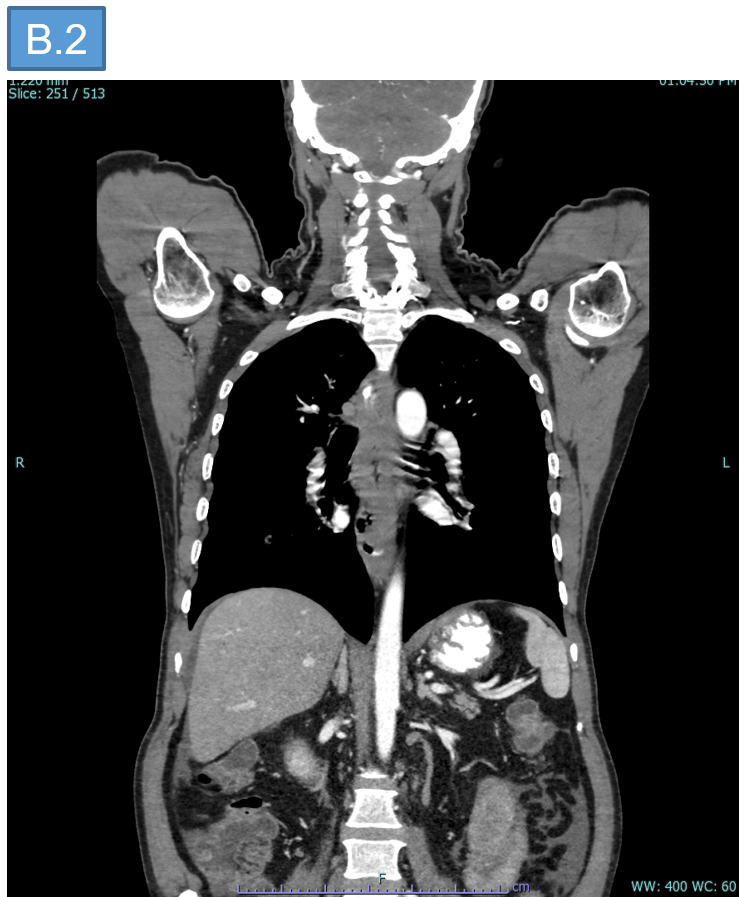
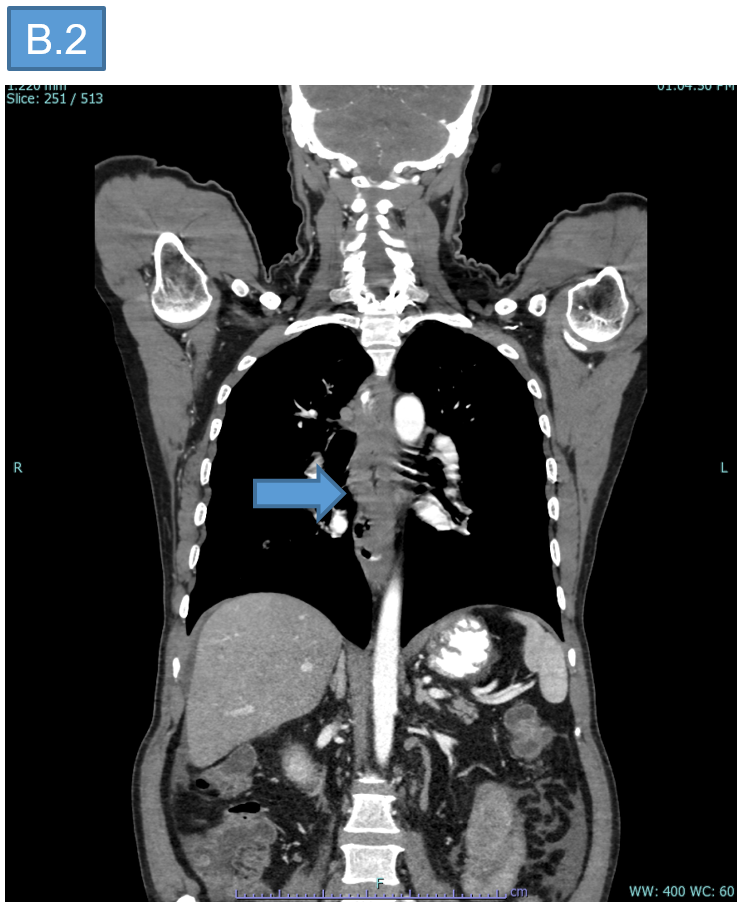
- B : CONTRAST ENHANCED CT
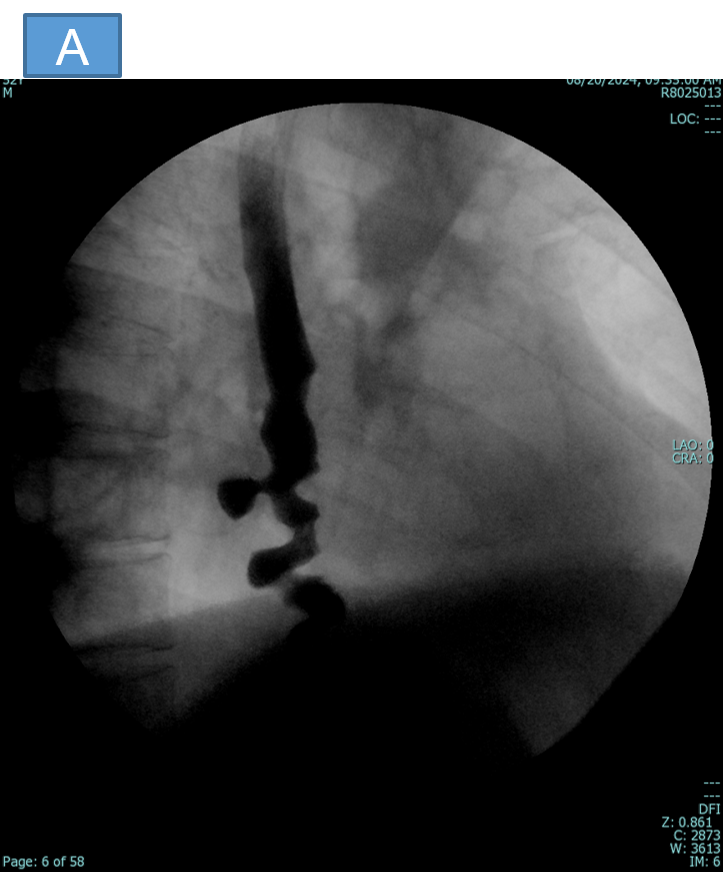

- A. Corckscrew oesophagus and diverticulum involving the distal oesophagus.
- B. Circumferential asymmetric hypo enhancing contiguous wall thickening involving the thoracic esophagus.
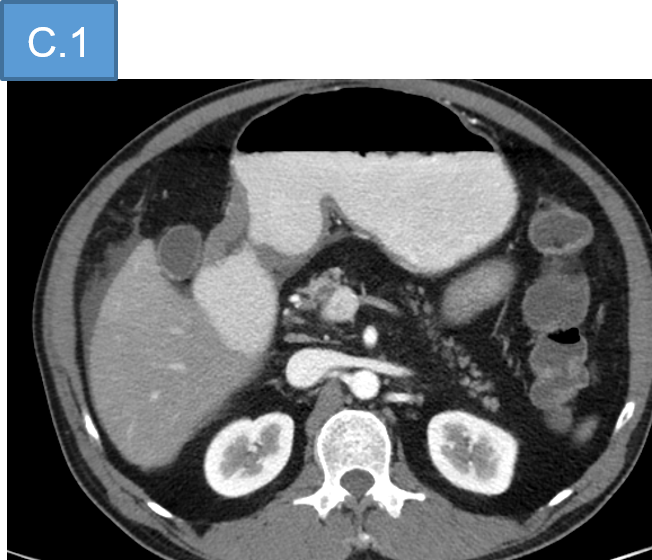
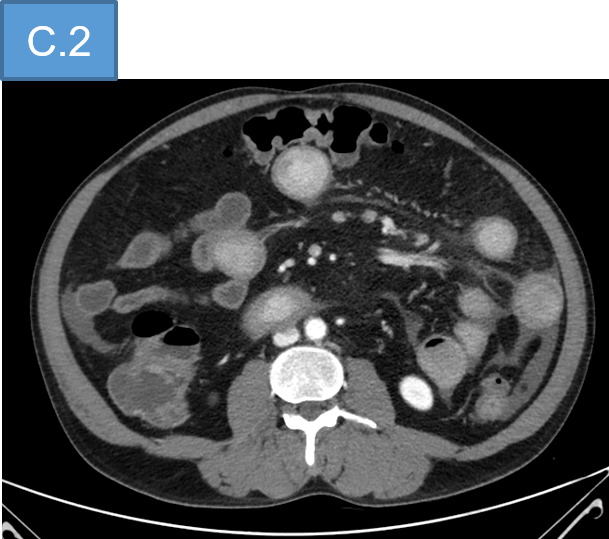
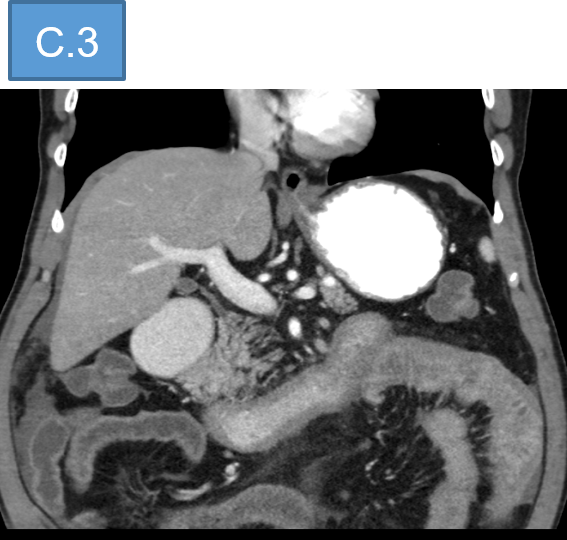
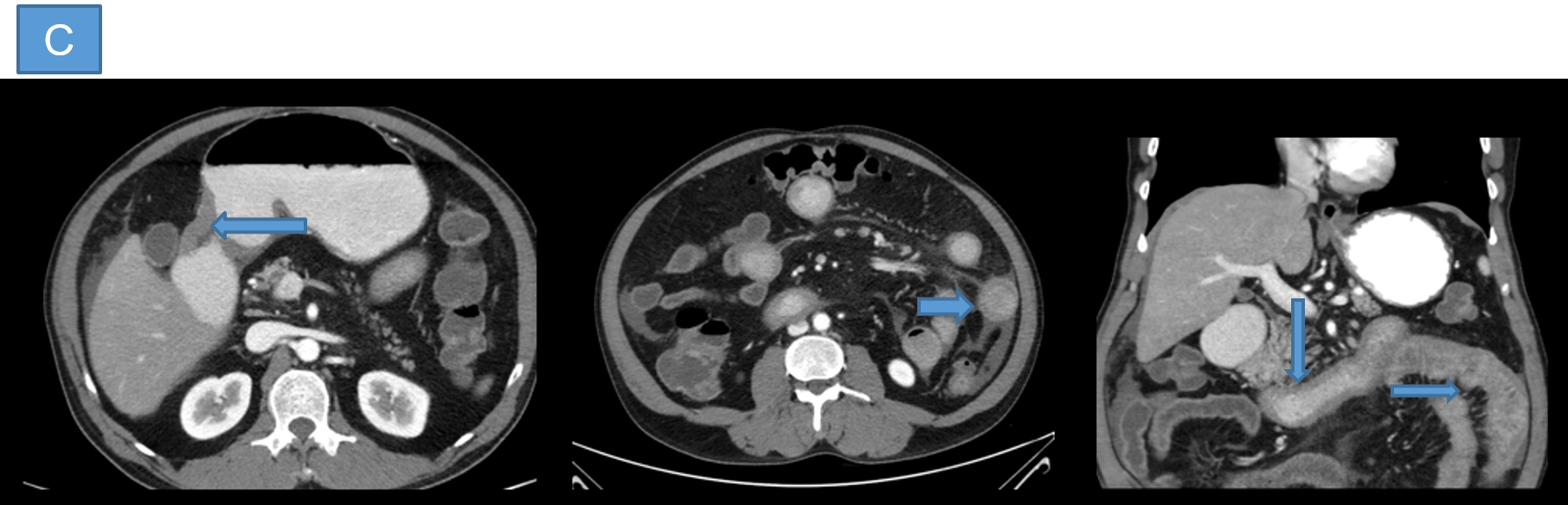
- C.
- Short segment plaque like wall thickening of the gastric antrum.
- Long segment, contiguous edematous wall thickening (Halo sign) involving the proximal small bowel loops with surrounding peri-enteric fat stranding.

DIAGNOSIS:
- Imaging features are suggestive of inflammatory etiology – likely Eosinophilic esophagitis with gastroenteritis. (Eosinophilic GI Disorders).
DISCUSSION:
- EGIDs can be primary or secondary EGIDs
- Primary EGIDs primarily affect the GI tract, with eosinophil-rich inflammation in the absence of known causes of eosinophilia such as parasitic infections, malignancy, and drug reactions.These EGIDs are associated with atopy and allergies and can be localized to one or more organs in the GI tract
- Secondary EGIDs - eosinophilic infiltration of the GI tract occurs in association with a separate known cause or identifiable systemic disease.
- The clinical symptoms of EGIDs are variable - a diagnostic evaluation for EGID is recommended for patients with refractory GI symptoms, especially those with a history of allergy-related diseases or a family history of EGIDs.
Eosinophilic esophagitis:
- Eosinophilic esophagitis (EoE) is the most common EGID
- EoE is a result of a complex interaction between immunogenetic factors and environmental exposure in predisposed individuals with atopy
- Esophagography is modality of choice for diagnosis and follow up.
- It allows real-time measurement of the esophageal diameter for stricture assessment and interventional planning
- The predominant pattern of EoE seen at esophagography is that of fixed luminal narrowing, which may be smooth and tapered or associated with characteristic ringlike indentations.
Eosinophilic Gastroenteritis:
- Eosinophilic infiltration of the stomach and small intestine
- A single bowel segment or multiple organs in various combinations also may be involved concurrently.
- Three subtypes of EGE according to the bowel layer involved.
- Mucosal – Mucosal thickening is the most prominent finding,
- Muscular -Bowel wall narrowing and dysmotility or obstruction
- Serosal - Ascites and may be accompanied by a thickened omentum and mesentery
- Imaging features resembles any other cause of gastroenteritis.
- Two signs have been described.
- Halo sign - layered gut wall appearance secondary to submucosal edema on contrast-enhanced cross-sectional images.
- The araneid limblike sign - when orally administered positive contrast material coats the thickened mucosal folds and sinks into the sinuses between the folds, resembling the appearance of spider legs.
- Neither of these signs is specific for eosinophilic enteritis, and both can be seen with several inflammatory and infective disorders.
- The diagnosis of EGID is based on clinical suspicion, supportive imaging findings, and histologic confirmation of eosinophil-rich inflammation in the tissue or organ.
- Management - Diet modification and use of oral corticosteroids
DIFFERENTIAL DIAGNOSIS:
- Any other causes of gastroenteritis (infective/ inflammatory)
Dr VIKHYATH SHETTY
Consultant Radiologist
Manipal Hospital, Yeshwanthpur, Bengaluru.
Dr DHINESHKUMAR
Radiology resident
Manipal Hospital, Yeshwanthpur, Bengaluru.
