
51 yr old female presented with chronic progressive ataxia.
- 51 yr old female presented with chronic progressive ataxia.
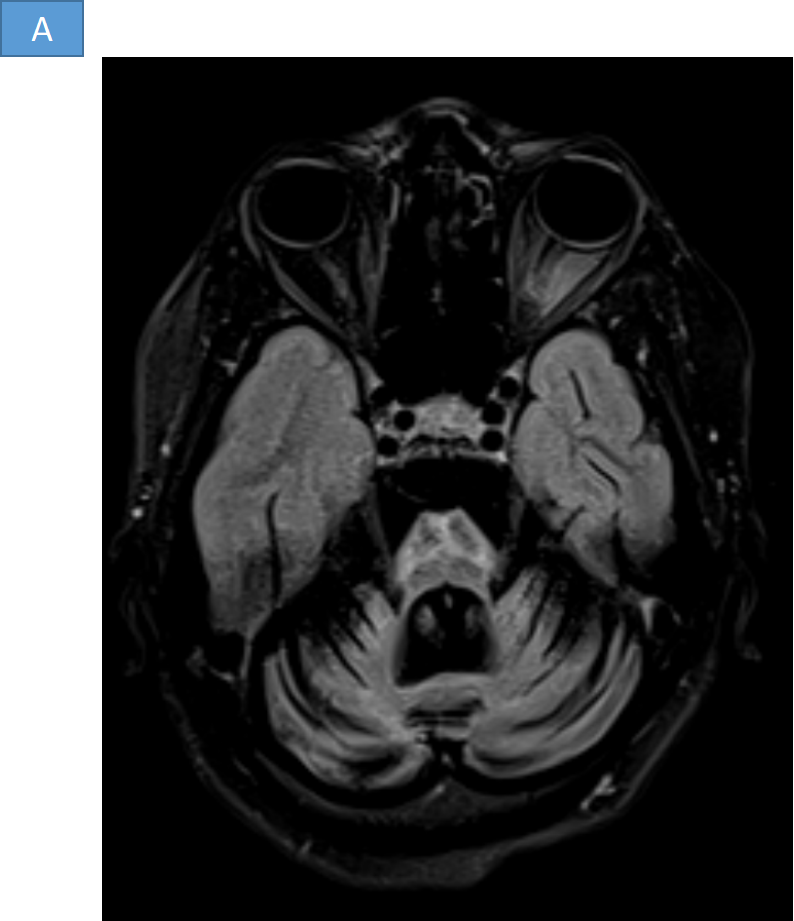
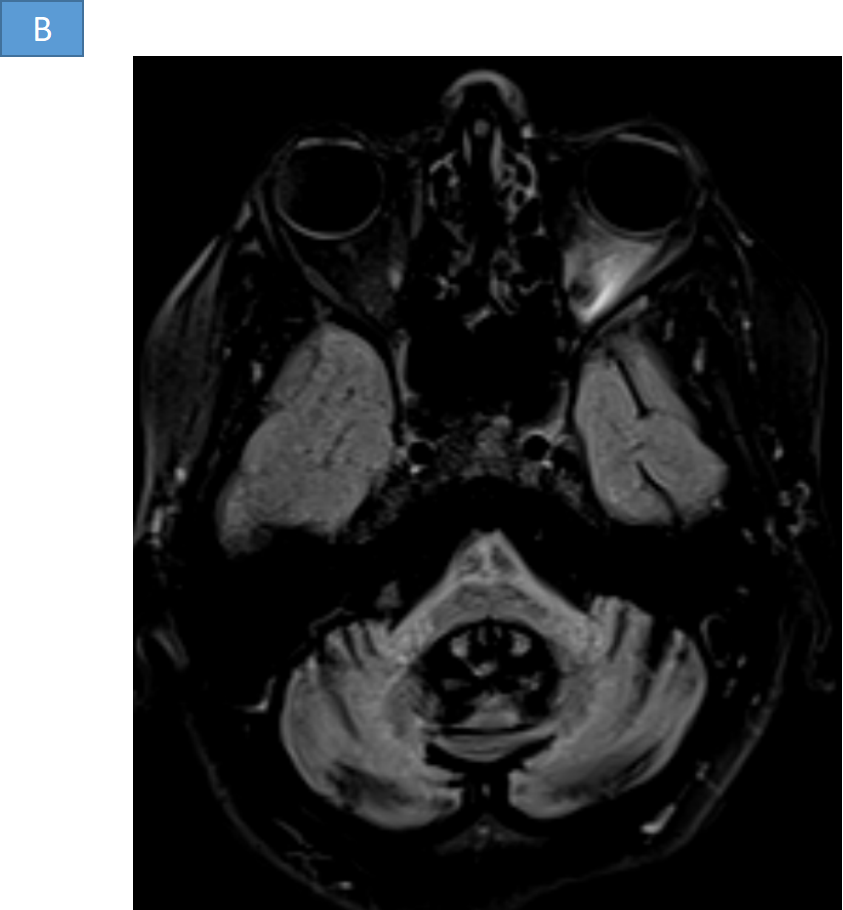
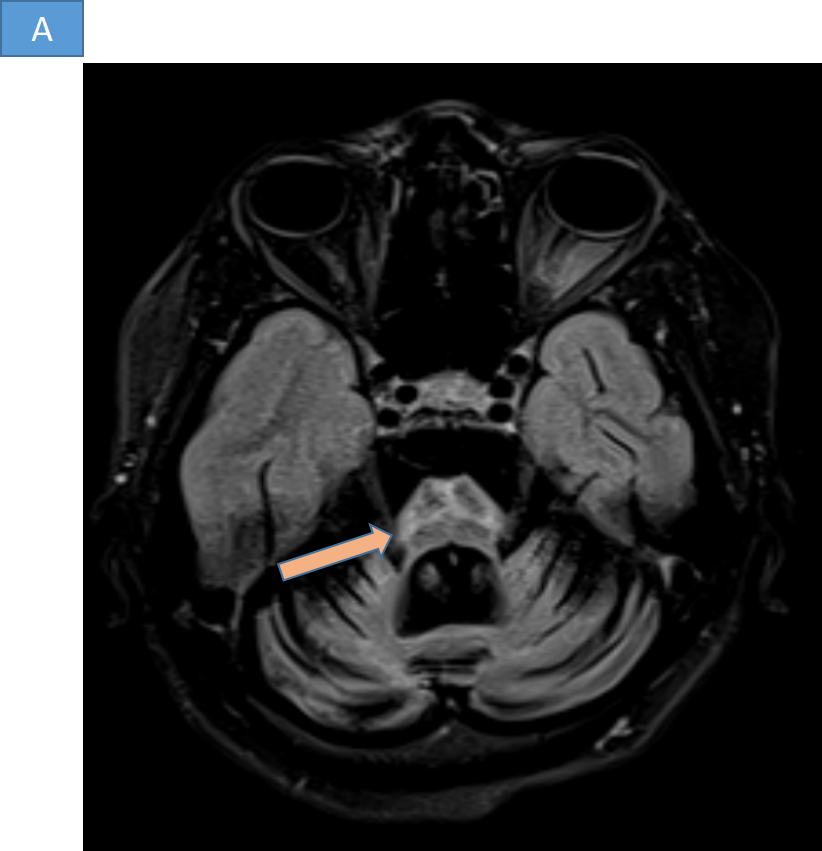
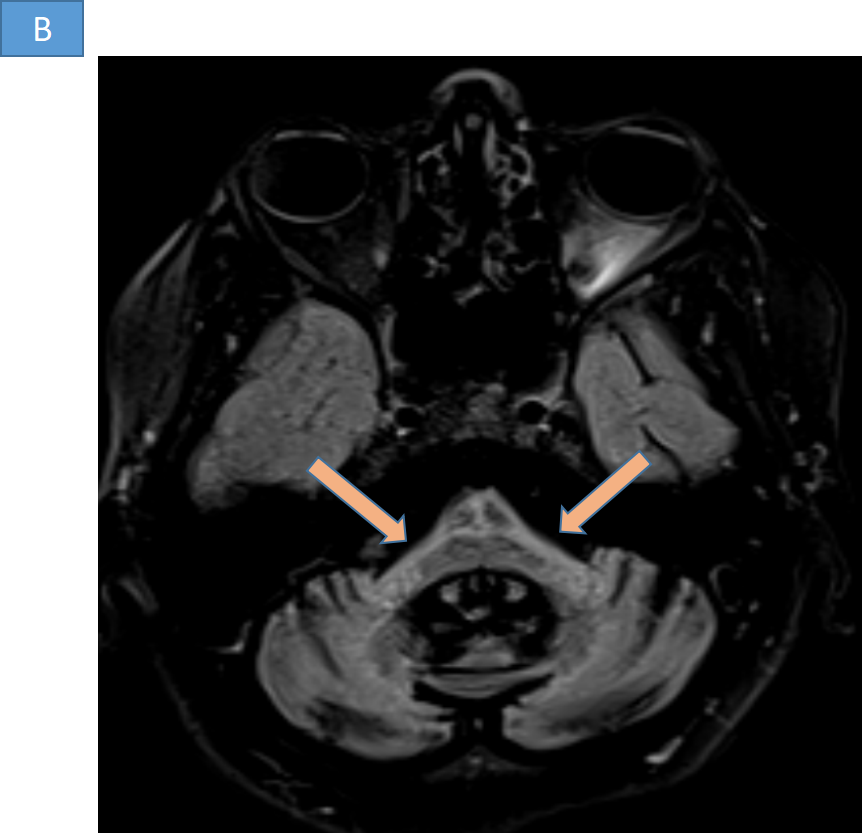
- A and B. Linear cruciform hyperintensity is seen in the pons resembling Hot cross bun sign. - Symmetric T2 hyperintense signals with atrophy of bilateral middle cerebellar peduncles.
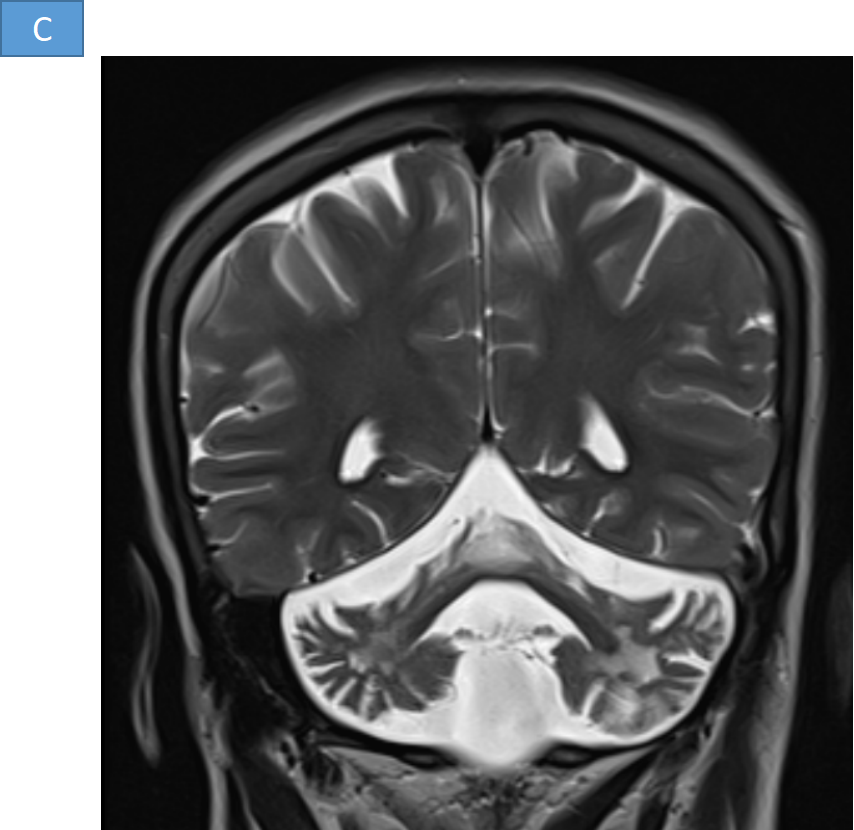
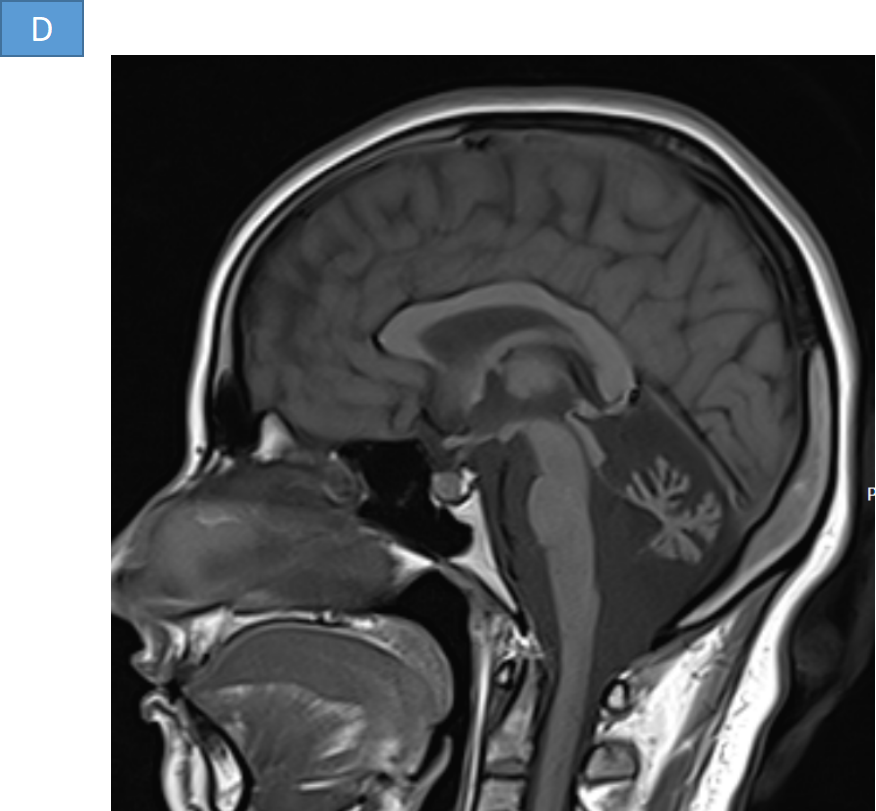
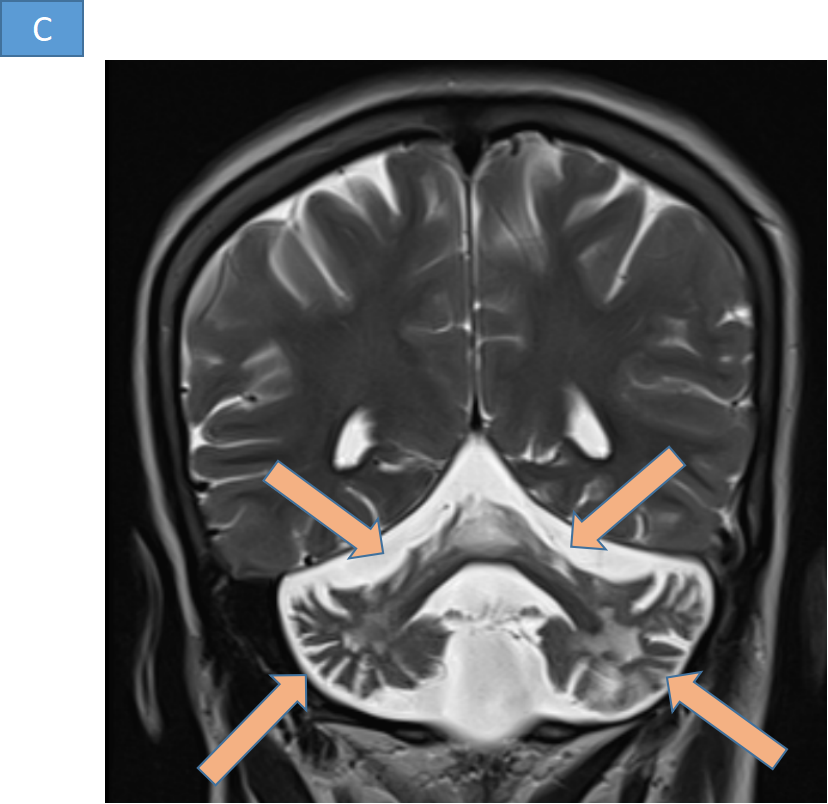
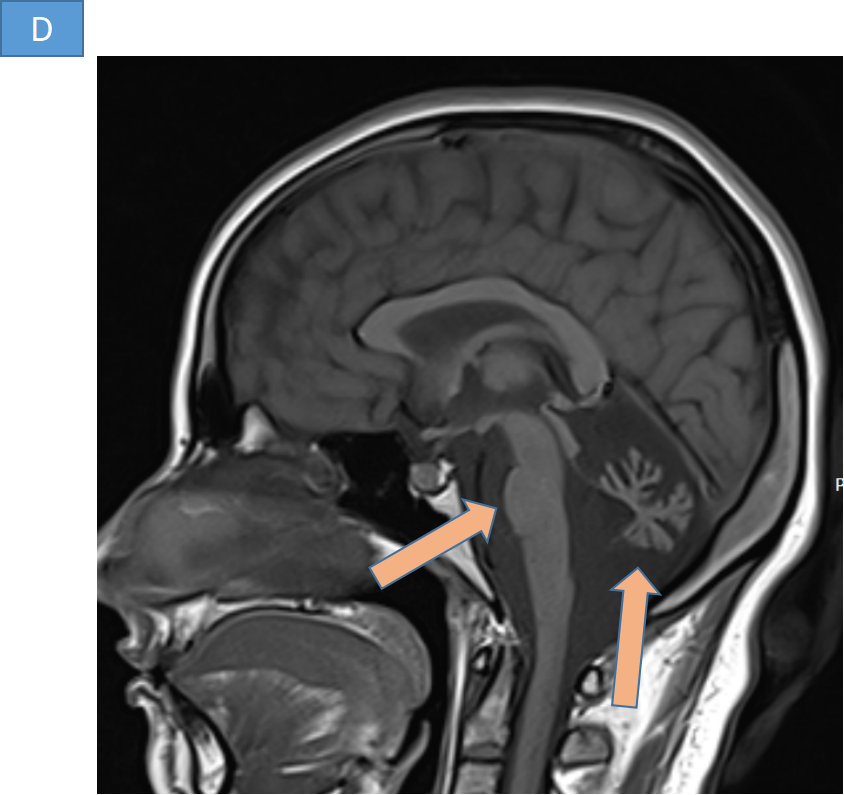
- C and D. - Significant atrophy of the bilateral cerebellar hemispheres, middle cerebellar peduncles and pons. There is ex vacuo prominence of the posterior fossa cisterns and fourth ventricle.
DIAGNOSIS
- MULTISYSTEM ATROPHY (TYPE C)
DISCUSSION
Multiple system atrophy (MSA)
- Adult-onset, progressive neurodegenerative disorder.
- Sporadic disease, with a prevalence of 4 per 100,000 .
- Symptoms typically begin between 40 and 60 years of age .
- Clinically they can present with parkinsonism, cerebellar ataxia, autonomic failure and pyramidal signs.
- Abnormalities of alpha-synuclein metabolism resulting in intracellular deposition.
- Pathological hallmark, argyrophilic aggregates in the cytoplasm of oligodendrocytes, termed glial cytoplasmic inclusions (GCIs).
- No effective treatment is currently available. The disease progresses relentlessly, culminating in death, usually within 10 years of diagnosis .
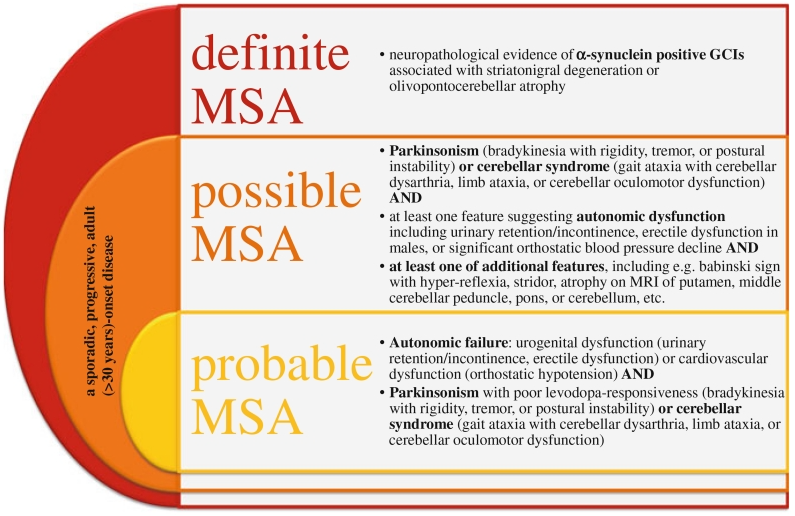
DIAGNOSIS OF MSA
Graded into 3 categories.
- Definite MSA
- Possible MSA
- Probable MSA
- “Definite” - only be used after postmortem pathological examination.
- “Probable MSA” - autonomic dysfunction, including otherwise unexplained urinary urgency, frequency, or incomplete emptying, erectile dysfunction in males, or orthostatic blood pressure drop by at least 30 mmHg systolic or 15 mmHg diastolic within 3 min of standing. As well, for a diagnosis of “probable MSA-P”, the patient must have a poorly levodopa-responsive parkinsonism (bradykinesia with rigidity, tremor, or postural instability), and for a diagnosis of “probably MSA-C”, the patient must have a cerebellar syndrome (gait ataxia with cerebellar dysarthria, limb ataxia, or cerebellar oculomotor dysfunction).
- “Possible MSA” - In the case that a patient has orthostatic hypotension not meeting the strict numerical criteria, if one of the additional suggestive features are present.
MSA TYPES
- Olivopontocerebellar atrophy: Cerebellar dysfunction predominates: MSA-C pattern.
- Striatonigral degeneration: Parkinsonian features predominates- MSA P pattern.
- Shy-Drager syndrome: Autonomic symptoms predominate- presentation with arterial orthostatic hypotension.
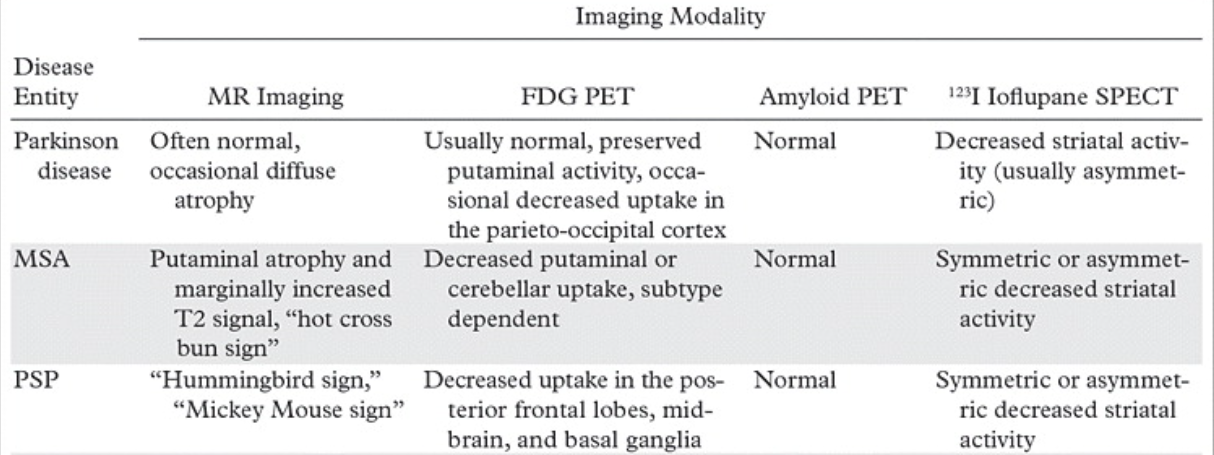
MRI
- T2 hyperintensities in the pontocerebellar tracts
- pons (hot cross bun sign) in MSA-C
- middle cerebellar peduncles
- Cerebellum
- Abnormal putaminal signal (in MSA-P) :
- reduced GRE and T2 signal relative to the globus pallidus and the red nucleus
- abnormally high T2 linear rim surrounding the putamen (putaminal rim sign) seen at 1.5 T (this is normal at 3 T)
- Disproportionate atrophy
- MSA-C: in cerebellum and brainstem (especially olivary nuclei and middle cerebellar peduncles)
- MSA-P: in putamen
Diffusion tensor imaging
- ADC: higher in the pons, cerebellum, and putamen compared with Parkinson disease or controls.
- fractional anisotropy (FA): lower in the pons, cerebellum, and putamen compared with Parkinson disease or controls.
Nuclear medicine
- On SPECT/CT with I-123 ioflupane, there is loss of the normal comma- or crescent-shaped tracer uptake in the striatum. Instead, a period- or oval-shaped uptake is seen within the caudate nucleus head, without tracer uptake in the putamen. Quantitative assessment reveals reduced uptake in the putamen compared with norms.
DIFFERENTIAL DIAGNOSIS
REFERENCES
- Fanciulli A, Stankovic I, Krismer F, Seppi K, Levin J, Wenning GK. Multiple system atrophy. International review of neurobiology. 2019 Jan 1;149:137-92.
- Bhattacharya K, Saadia D, Eisenkraft B, Yahr M, Olanow W, Drayer B, Kaufmann H. Brain magnetic resonance imaging in multiple-system atrophy and Parkinson disease: a diagnostic algorithm. Archives of neurology. 2002 May 1;59(5):835-42.
- Palma JA, Norcliffe-Kaufmann L, Kaufmann H. Diagnosis of multiple system atrophy. Autonomic Neuroscience. 2018 May 1;211:15-25.
- Kim HJ, Jeon B, Fung VS. Role of magnetic resonance imaging in the diagnosis of multiple system atrophy. Movement Disorders Clinical Practice. 2017 Jan;4(1):12-20.
- Zhu S, Deng B, Huang Z, Chang Z, Li H, Liu H, Huang Y, Pan Y, Wang Y, Chao YX, Chan LL. “Hot cross bun” is a potential imaging marker for the severity of cerebellar ataxia in MSA-C. NPJ Parkinson's disease. 2021 Feb 15;7(1):15.
Dr. SRIRAM PATWARI
SENIOR CONSULTANT
MANIPAL HOSPITAL , YESHWANTHPUR, BENGALURU
Dr. JOMON SUNNY
FELLOW IN CROSS SECTIONAL IMAGING
MANIPAL HOSPITAL , YESHWANTHPUR, BENGALURU

