
50-year-old gentleman with pain in abdomen and fever for 5 days
A 50-year-old gentleman with pain in his abdomen and fever for 5 days
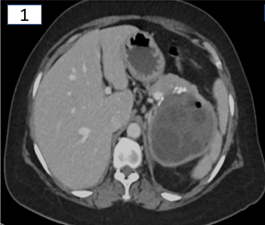
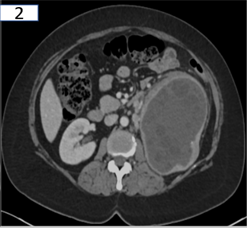


- There is thick peripherally enhancing cystic lesion centered in upper pole of left kidney withmultiple rounded daughter cysts noted within at the periphery. Fewpunctate calcifications seen in the cystic wall. (fig.1 and 2)
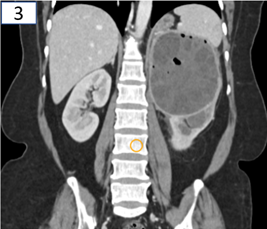
- Multiple internal air fociand enlarged nodes are also noted. (fig.3)
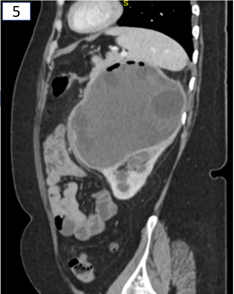
- Focal defect in the inferior aspect of the cyst communicating the dilated upper pole calyx. (fig.4 and 5)
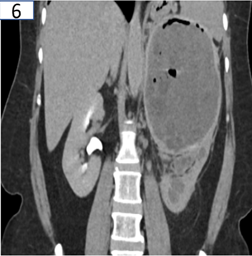
- No excretion of contrast seen in left collecting system in delayed phases. (fig.6)
- Mild dilatation of the left collecting system and the proximal ureter with hydatid cysts seen within, causing ipsilateral proximal obstructive uropathy (fig.7)
DIAGNOSIS:
Infected left renal hydatid cyst ruptured into the left pelvicalyceal system with obstructive uropathy.
DISCUSSION:
RENAL HYDATID:
- It is very rare manifestation ofhydatid disease. Seen in less than 5%. The most common manifestations of renal hydatid disease are flank mass, pain, and dysuria.
- Infection is caused by Echinococcus tapeworm. The life cycle of E granulosus involves two hosts: a definitive host, usually a dog and an intermediate host, most commonly a sheep
- The liver (75% of cases) and lung (15% of cases) are most affected by hydatid disease.
- The wall of a hydatid cyst comprises three layers. The outermost layer, or pericyst, the middle, laminated membrane and the inner, germinal layer.
- Imaging appearances vary with the development of the parasite, and three types of cysts may be distinguished: Type 1 cysts correspond to the initial developmental stage of the parasite and appear unilocular, without internal architecture; type 2 cysts are seen at an intermediate stage of parasitic development and contain multiple daughter cysts; and type 3 cysts are completely calcified and represent the death of the parasite.
- Plain radiograph: soft-tissue mass or a ring-shaped calcification in the renal region.
- Ultrasound: anechoic lesions with well-defined margins. The “falling snowflake” or “snowstorm” sign—multiple echogenic foci produced by hydatid sand that is dispersed when the patient rolls—is pathognomonic of hydatid disease.
- CT shows unilocular or multilocular cysts with or without peripheral calcifications. It may also show a detachment of the endocyst from the pericyst with a “floating membranes” appearance, a multiloculated cyst with mixed internal density, and daughter cysts with lower density than the maternal matrix.2,4,5
- The presence of air with or without air fluid/ fluid fluidlevels within a hydatid cyst are suggestive of infection.5
- Treatment is primarily surgical and consists of total or partial nephrectomy.
References:
- Haaga JR, Boll D. CT and MRI of the whole body. Mosby. (2009) ISBN:0323053750.
- Polat P, Kantarci M, Alper F, Suma S, Koruyucu MB, Okur A Hydatid disease from head to toe. RadioGraphics 2003;23(2):475–494
- Rami M, Khattala K, Elmadi A et-al. The renal hydatid cyst: report on 4 cases. Pan Afr Med J. 2012;8: 31.
- Beggs I The radiology of hydatid disease. AJR Am J Roentgenol 1985;145(3):639–648
- Mehta P, Prakash M, Khandelwal N. Radiological manifestations of hydatid disease and its complications. Trop Parasitol. 2016;6(2):103-112. doi:10.4103/2229-5070.190812
Dr Sunita Gopalan
DMRD, FRCR
Senior Consultant Radiologist
Columbia Asia Radiology Group
Dr Ankur Chandra,
MDRD
Cross-sectional fellow,
Columbia Asia Whitefield
