5-month-old male baby Presented to ER with acute onset of episodic cries, and vomiting
- 5 month old male baby Presented to ER with acute onset of episodic cries, and vomiting.
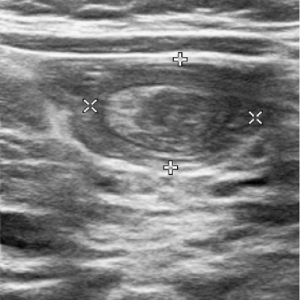
- Ultrasound examination of abdomen and pelvis was performed.
Bowel within bowel appearance of intussusception, with thick walled cystic lesion inthe mid upper abdomen as the lead point of intussusception.
- 5 month old male baby Presented to ER with acute onset of episodic cries, and vomiting.
- Ultrasound examination of abdomen and pelvis was performed.
Bowel within bowel appearance of intussusception, with thick walled cystic lesion inthe mid upper abdomen as the lead point of intussusception.


- Pneumatic reduction of the intussusception under fluoroscopic guidance was performed.
- The child returned within 24 hours with similar complaints and ultrasound examination revealed recurrent intussusception.
- Intussusception was reduced and CT examination was performed for evaluation of the cystic lesion that was acting as a lead point.
Well-defined spherical cystic lesion of uniform fluid attenuation and thin enhancing walls in the left lumbar region. No enhancing internal septations or solid component.


- Diagnosis of enteric duplication cyst acting as a lead point for recurrent intussusception was suggested.
- In view of recurrent intussusception and risk of further recurrence, child underwent RUQ laparotomy + excision of distal Ileum bearing intraluminal duplication cyst + end-to end ileal anastomosis + appendectomy.
- Diagnosis of enteric duplication cyst acting as a lead point for recurrent intussusception was suggested.
- In view of recurrent intussusception and risk of further recurrence, child underwent RUQ laparotomy + excision of distal Ileum bearing intraluminal duplication cyst + end-to end ileal anastomosis + appendectomy.
Intra-operative pictures

DISCUSSION:
- Enteric duplication cysts (EDCs) – congenital malformations formed during the embryonic development of the digestive tract.
- Can develop anywhere along the gastrointestinal tract, ileum being the most frequent localization.
- Prevalence: 1:4,500 births. Slight male predominance.
- Majority of duplication cysts present clinically at pediatric age, mostly within 2 years of life (80%).

- Characteristically arise from the mesenteric border of the intestine.
- Contain a layer of smooth muscle tissue and share a common wall with the GI tract, but no communication with GI tract lumen.
- The anatomical structure resemble the enteric stratification and the mucosal layer can include ectopic gastric tissue and, less commonly, pancreatic.
- Technetium Tc 99m scintigraphy can detect ectopic gastric mucosa.
Treatment and prognosis:
- EDCs tend to increase in size gradually and can cause complications such as obstruction, massive bleeding or even a potential risk for malignant transformation in the adulthood – making surgical excision necessary
- Cyst excision alone or if there is a communication, resection of the adjacent bowel is necessary.
- It is important to ensure that the cyst is entirely resected because recurrence or malignant changes may occur.
REFERENCE:
- Sangüesa Nebot C, Llorens Salvador R, Carazo Palacios E, Picó Aliaga S, Ibañez Pradas V. Enteric duplication cysts in children: varied presentations, varied imaging findings. Insights into imaging. 2018 Dec;9(6):1097-106.
- Fonseca EK, Sameshima YT. Gut signature sign in enteric duplication cysts. Abdominal Radiology. 2018 Dec 1;43(12):3513-4.
- D’Agostino V, Castaldo A, Catelli A, Pesce I, Genovese S, Coppola L, Monaci A, Esposito C, Amitrano M. An ileal duplication cyst case report: From diagnosis to treatment. Radiology Case Reports. 2021 Jul 1;16(7):1597-602.
Dr Rashmi Jayakar Poojary
Primary DNB Radiology Resident
Manipal Hospital Yeshwanthpur
Dr. Vikhyath Shetty
Consultant Radiologist
Manipal Hospital Yeshwanthpur
Dr Sai Prasad
Senior Pediatric Surgeon
Manipal Hospital Yeshwanthpur