
48-year-old female with complaints of bilateral diminished vision and headache
A 48-year-old female with complaints of bilateral diminished vision and headache.
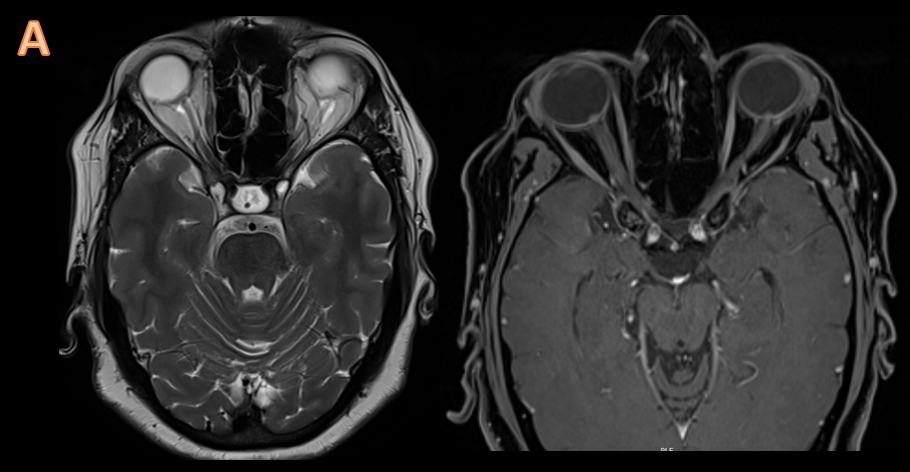
Optic nerves
- Prominent subarachnoid space around the optic nerves
- Vertical tortuosity of the optic nerves
- Flattening of the posterior sclera
- Intraocular protrusion of the optic nerve head
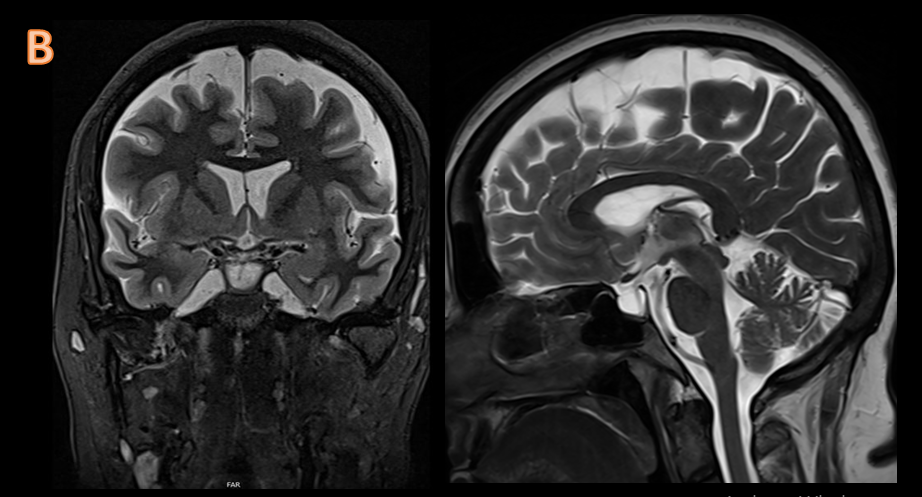
Enlarged arachnoid outpouchings
- Partially empty sella turcica
- Enlarged Meckel cave
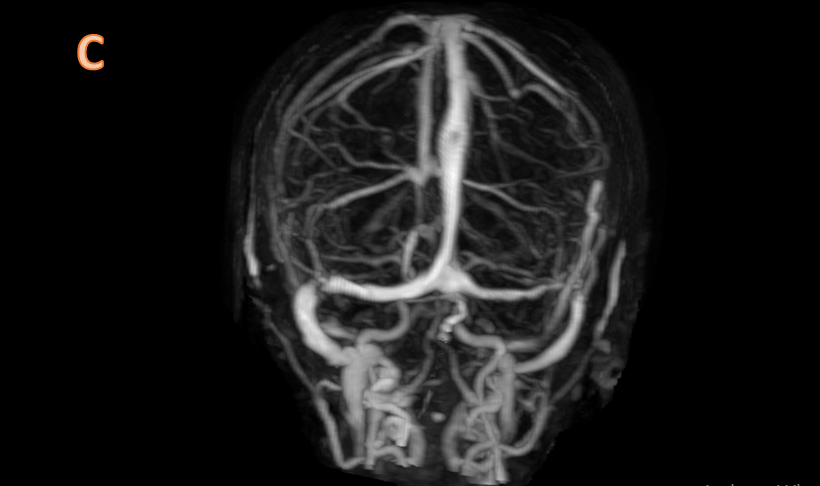
Bilateral venous sinus stenosis
- Lateral segments of the transverse sinuses
DIAGNOSIS:
IDIOPATHIC INTRACRANIAL HYPERTENSION
DISCUSSION:
- Idiopathic intracranial hypertension (IIH) is a headache syndrome characterized by raised CSF pressure in the absence of an intracranial mass lesion or ventricular dilation; normal CSF composition; usually normal results of neurologic examination, except for papilledema and occasional CN VI palsy.
- The hallmark of IIH is papilledema, which may be bilateral, asymmetrical, or even unilateral; however, IIH can occur in the absence of papilledema.
- Associations include endocrine causes(adrenal insufficiency, Cushing disease, hypoparathyroidism, hypothyroidism, excessive thyroxine replacement in children), drugs(doxycycline), chronic renal failure, systemic lupus erythematosus (SLE), hypervitaminosis A(in the pediatric population), dural venous sinus stenosis or web: rare but treatable cause of IIH
- The presentation is usually with headaches, visual problems (transient or gradual visual loss), pulse-synchronous tinnitus, photopsia and eye pain.
- In the absence of a cause for raised intracranial pressure, imaging features that support the diagnosis of idiopathic intracranial hypertension include: prominent perioptic subarachnoid spaces,vertical tortuosity of the optic nerves, flattening of the posterior sclera, intraocular protrusion of the optic nerve head and enhancement of the intraocular)optic nerves. There is associated enlarged arachnoid outpouchings in the form of partially empty sella, enlarged Meckel cave, aberrant arachnoid granulations/small meningoceles typically within the temporal bone and sphenoid wing. There can be bilateral venous sinus stenosis particularly along the lateral segments of the transverse sinuses
- Differentials include venous sinus thrombosis, Chiari I malformation, Other causes of intracranial hypertension and papilledema.
Dr. Sriram Patwari
MD, PDCC (Neuroradiology), EDiNR
Consultant Radiology, Co-lead Neuroradiology
Manipal Hospitals Radiology Group
Dr. Naveen SS
Cross Sectional Imaging Fellow
Manipal Hospitals Radiology Group
