
46 Year old female patient presents with right iliac fossa and supraumbilical pain, loose stools
- 46 Year old female patient presents with right iliac fossa and supraumbilical pain, loose stools.
- K/c/o Endometriosis.
- USG- Cholelithiasis. Umbilical hernia.
- CT was advised.
FINDINGS- CT ABDOMEN AND PELVIS WITH IV CONTRAST
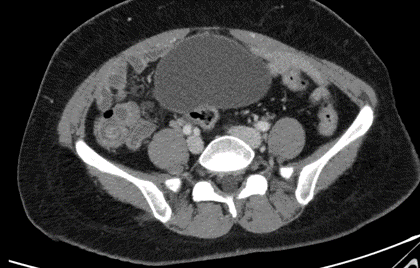
- A.Axial and coronal venous phase images
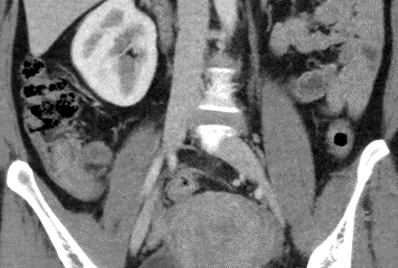
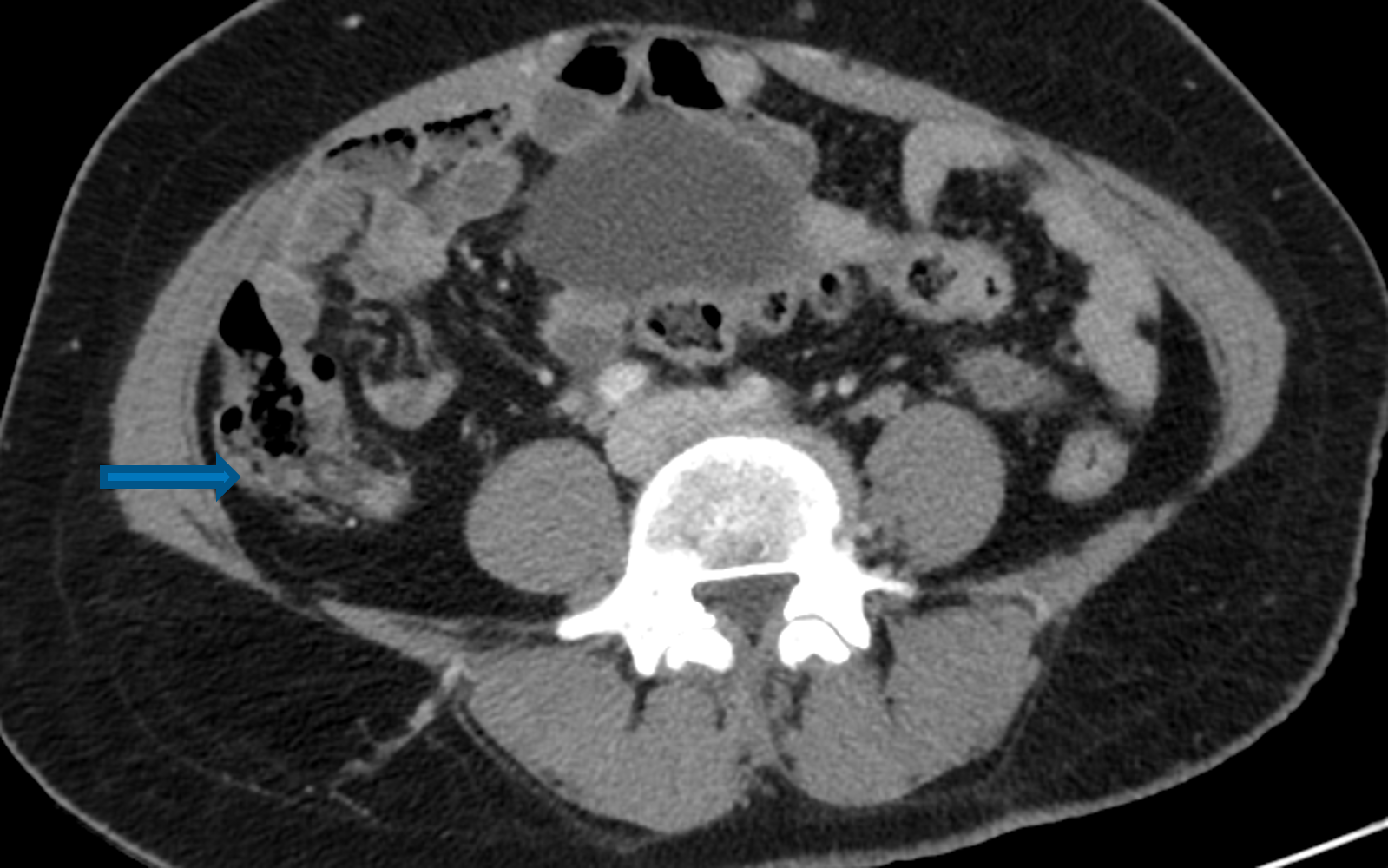
- B. Coronal and axial venous phase images


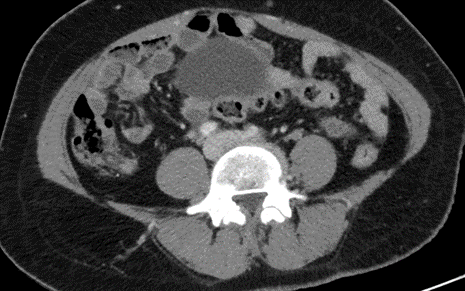
- A. Axial and coronal venous phase images
- Appendico-cecal invagination of proximal part of appendix showing bowel within bowel appearance.
- B. Coronal and axial venous phase images
- Terminal ileum and Ileocecal juntion is normal.



Appendiceal intussusception.
Patient underwent Open Partial Right Hemicolectomy / Laparoscopic Cholecystectomy
HPE:
Partial right hemicolectomy: Multiple foci of endometriosis, acute on chronic inflammation of appendix with intussusception.
DISCUSSION
- Appendiceal intussusception is very rare condition with an estimated incidence of 0.01%.
- Usually asymptomatic or complaints similar to appendicitis or intussusception.
Causes
- Can occur without any underlying abnormality
- Anatomical variations of the appendix and pathological conditions such as tumors or polyps, endometriosis, parasitism, cystic fibrosis, appendicoliths and foreign bodies
Preoperative diagnosis is accomplished with computed tomography (CT) or ultrasonography, but the diagnosis is very difficult, and many cases are diagnosed during or after surgery
US
- Children,
- Longitudinal sonograms may show the inverted appendix protruding into the cecal lumen.
- Target sign (also known as the doughnut sign)
- Pseudokidney sign
- Crescent in a doughnut sign
CT
- CT scan can clearly show the appendix invaginated into the cecal lumen.
- The presence of a concentric central mass (target-like sign) can be helpful for diagnosis
Differential diagnosis
- Cecal tumor
- Ileocecal intussusception
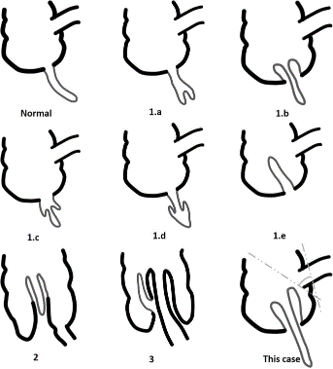
Classification
- 1.a – invagination of the appendiceal tip into the proximal appendix
- 1.b – invagination beginning at the junction of the appendix and the cecum
- 1.c – invagination beginning along the length of the appendix
- 1.d – retrograde intussusception of the proximal appendix into the distal appendix
- 1.e – complete invagination of the appendix into the cecum
- 2 – compound intussusception- secondary intussusception of the cecocolic type induced by invaginated appendix as a apex with an appendiceal intussusception
- 3 – any type of appendiceal intussusception complicated by an ileocolic intussusception
- 4 – invagination of an appendiceal mucocele into the cecum
- In types 1.a, 1.c, and 1.d -appendectomy is sufficient because the lesion does not include the appendiceal base
- In types 1.b and 1.e - partial cecectomy should be considered first
- In type 2 - even though the intussusception can be reduced, it is advisable to perform a partial cecectomy first
- In type 3 - we should identify the origin of the ileocecal intussusception and remove the trigger point
- In type 4 - if the malignant potential seems to be low or equivocal, the lesion can be managed similarly to types 1.b, 1.e, 2 and 3. However, if malignancy is strongly suspected based on the preoperative evaluation or during surgery, a right hemicolectomy
Dr MADHUKUMAR,
Senior Consultant Radiologist
Manipal hospital, Yeshwanthpur, Bengaluru.
Dr. DHINESHKUMAR T
Radiology resident
Manipal hospital, Yeshwanthpur, Bengaluru.

