
44 year old gentleman Presented in ER with fever, epigastric pain radiating to the back since one day
- 44 year old gentleman Presented in ER with fever, epigastric pain radiating to the back since one day
- O/E – P/a diffuse tenderness
- Lab: Elevated s.amylase/lipase
Raised TC

FINDINGS
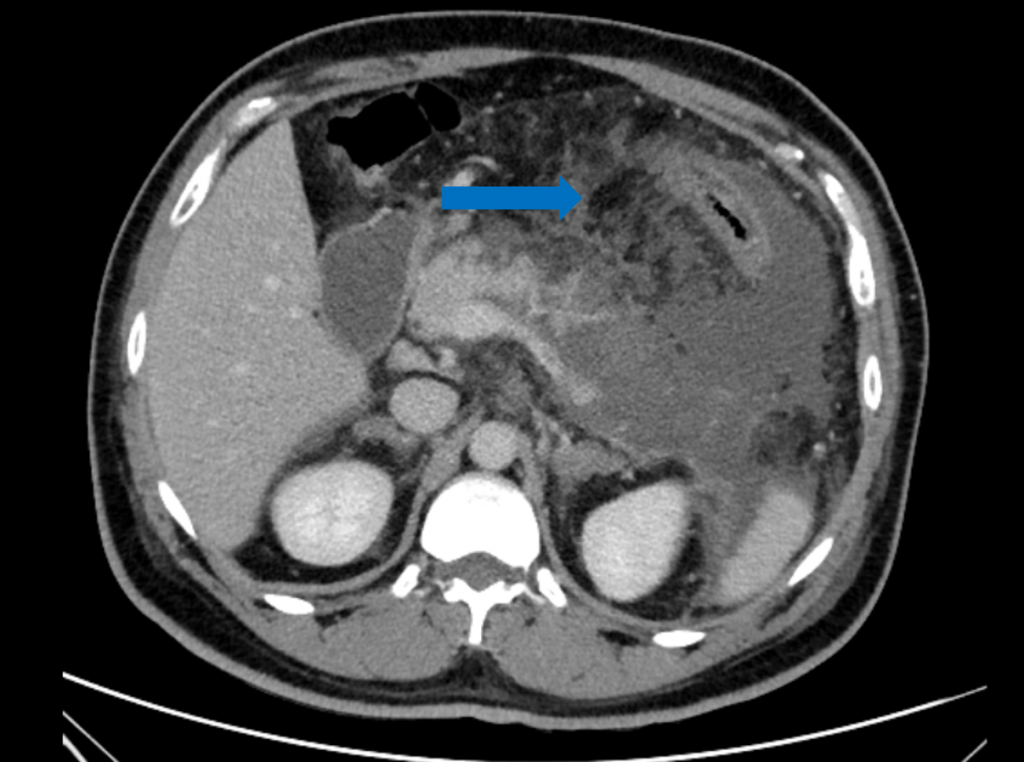
- A – Axial CECT demonstrating significant peripancreatic fluid and fat stranding (blue arrow) with non-enhancing pancreatic body and tail suggestive of acute necrotising pancreatitis.
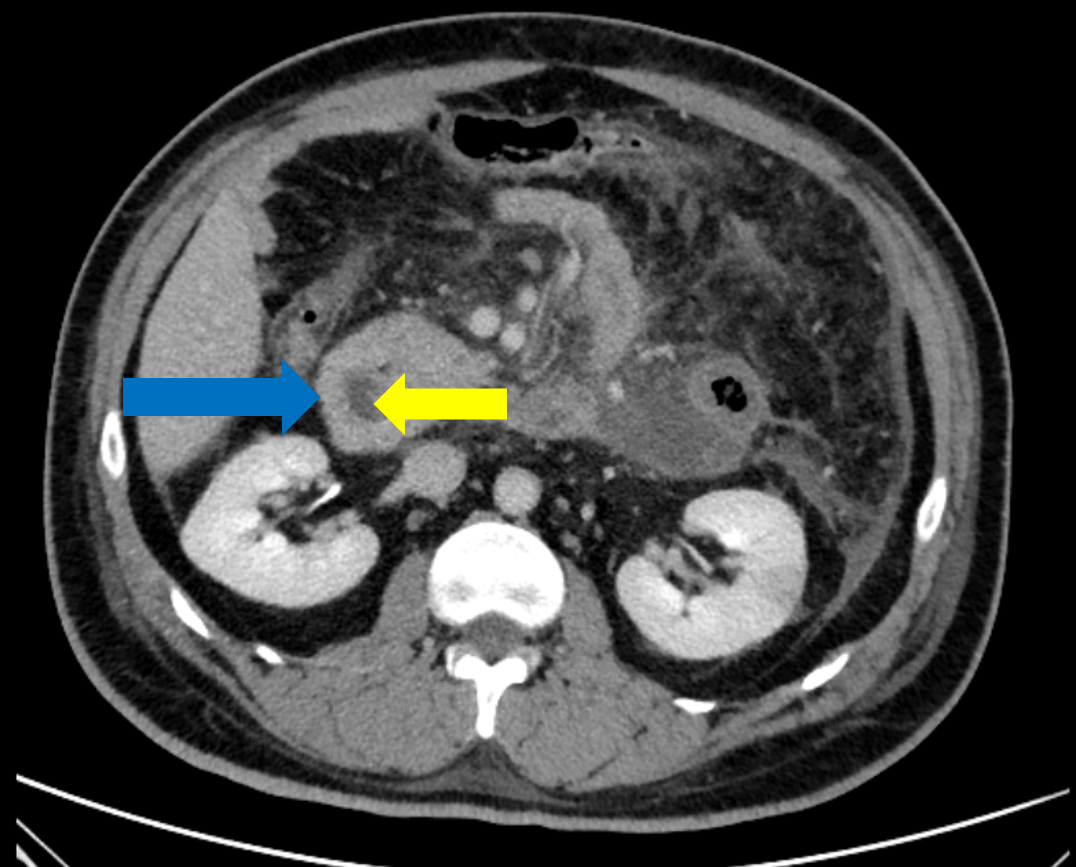
- B – Axial CECT showing circumferential enhancing soft tissue (blue arrow) encasing the second part of duodenum (yellow arrow)– complete annular pancreas.
- C – Coronal CECT showing dilation of third part of duodenum with a thin elongated intraluminal structure (blue arrow) within – intraluminal duodenal diverticulum.
Diagnosis:
- ACUTE NECROTIZING PANCREATITIS WITH ANNULAR PANCREAS AND INTRALUMINAL DUODENAL DIVERTICULUM
Annular pancreas
- The pancreas develops from a single dorsal and two ventral buds, which appear as outgrowths of primitive foregut at 5 weeks of gestation. In the 7thweek of gestation, the duodenum expands and rotates the ventral bud from right to left which then fuses with the dorsal bud. The ventral bud forms the inferior part of uncinate process and inferior head of pancreas while the dorsal bud gives rise to the tail and body of pancreas.
- Annular pancreas develops due to failure of the ventral bud to rotate with the duodenum, causing encasement of the duodenum.
- Two types: complete/incomplete
- Complications: Pancreatitis, duodenal obstruction, rarely biliary obstruction
- Management: surgery in symptomatic cases Duodenojejunostomy, gastojejunostomy
Duodenal web/diverticulum
- Represents delayed manifestation of a congenital duodenal web or diaphragm, which results from incomplete recanalization of midgut during the 6th-8th weeks of embryologic life.This duodenal diaphragm with its small central orifice will gradually protrude distally into the duodenal lumen as a mucosal pocket, like a windsock, because of the peristaltic pressure and intraluminal content.
ASSOCIATION – Down syndrome, Annular pancreas, Intestinal malrotation, potassium supplementation, NSAIDs.
FLUOROSCOPIC SIGNS:
- Windsock sign
- Duodenal dimple sign
COMPLICATIONS: duodenal obstruction, peptic ulcer disease, gastrointestinal hemorrhage, pancreatitis, and cholangitis
TREATMENT: Symptomatic patients can be treated surgically or endoscopically, with endoscopy being the preferred approach since it is less invasive. Endoscopic treatment consists of either diverticulotomy with needle-knife incision or diverticulectomy via snare resection
WINDSOCK SIGN
COMPANION CASE



DUODENAL DIMPLE SIGN


REFERENCE:
- Berrocal T, Torres I, Gutiérrez J et-al. Congenital anomalies of the upper gastrointestinal tract.
- Rha SE, Lee JH, Lee SY et-al. Duodenal diaphragm associated with long-term use of nonsteriodal antiinflammatory drugs: a rare cause of duodenal obstruction in an adult. AJR Am J Roentgenol. 2000;175 (3): 920
- Borghei, Peyman; Sokhandon, Farnoosh; Shirkhoda, Ali; Morgan, Desiree E. (2013). Anomalies, Anatomic Variants, and Sources of Diagnostic Pitfalls in Pancreatic Imaging. Radiology, 266(1), 28–36.
Dr. Madhu Kumar
Senior Consultant Radiologist
Manipal Hospital, Yeshwanthpur, Bengaluru.
Dr. Vikhyath Shetty
Consultant Radiologist
Manipal Hospital, Yeshwanthpur, Bengaluru.
Dr. Anagh Vishnu Narayanan
Radiology resident
Manipal Hospital, Yeshwanthpur, Bengaluru.
Dr. Priyanka
Radiology resident
Manipal Hospital, Yeshwanthpur, Bengaluru.

