39 years female with complains of heart burn and abdominal distension for one year
- 39 years female with complaints of heart burn and abdominal distension for one year.
- Recurrent episodes of nonbilious vomiting containing food particles.
- OGD scopy demonstrated food stasis in the stomach; hyperemic mucosa with multiple erosions in the stomach and tight stricture in D1.


FINDINGS
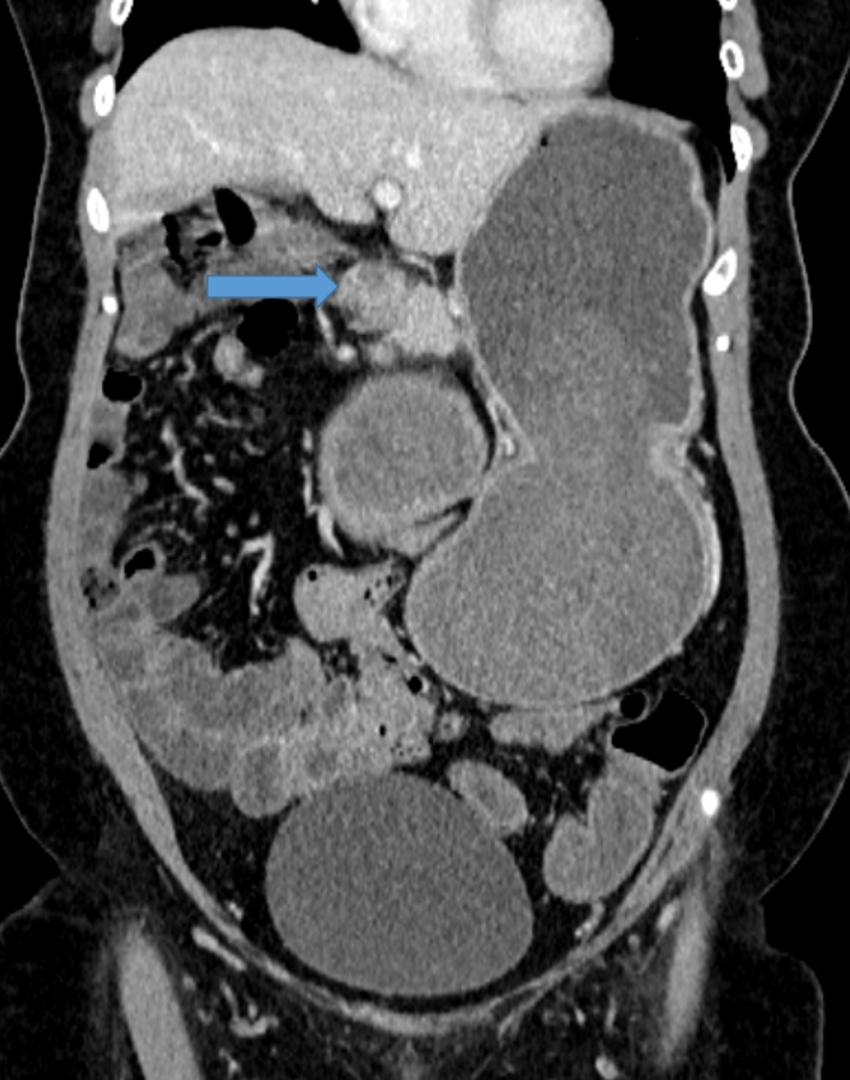
FIG 1A: Coronal venous phase images showing grossly dilated stomach fluid-filled stomach upto level of pylorus. No significant wall thickening or inflammatory changes.
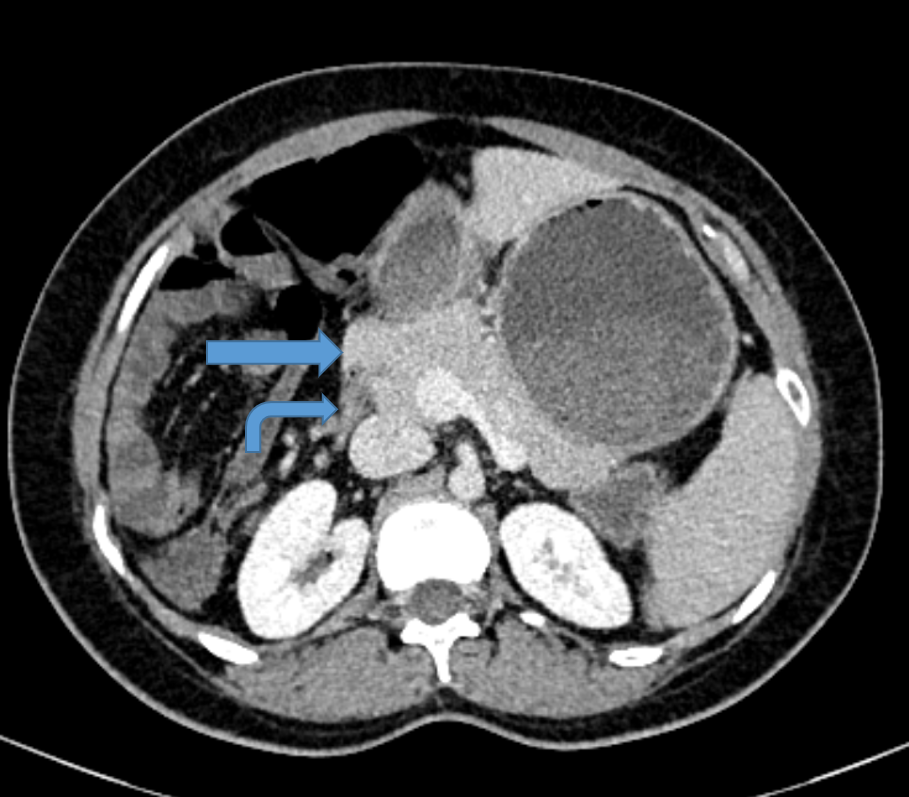
FIG 1B: Axial and coronal sections showing head of the pancreas partially encircling inferior duodenum at junction of D1 and D2. Distally the duodenum is collapsed (curved arrow).
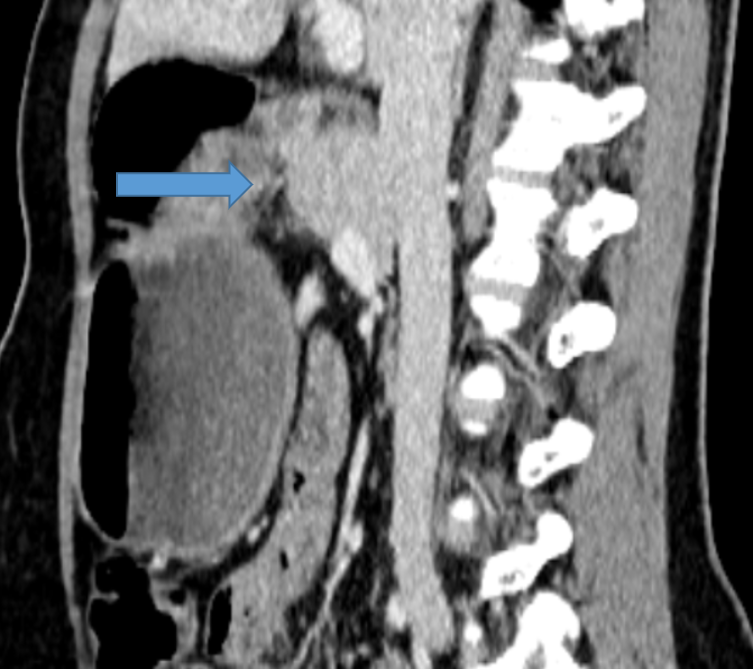
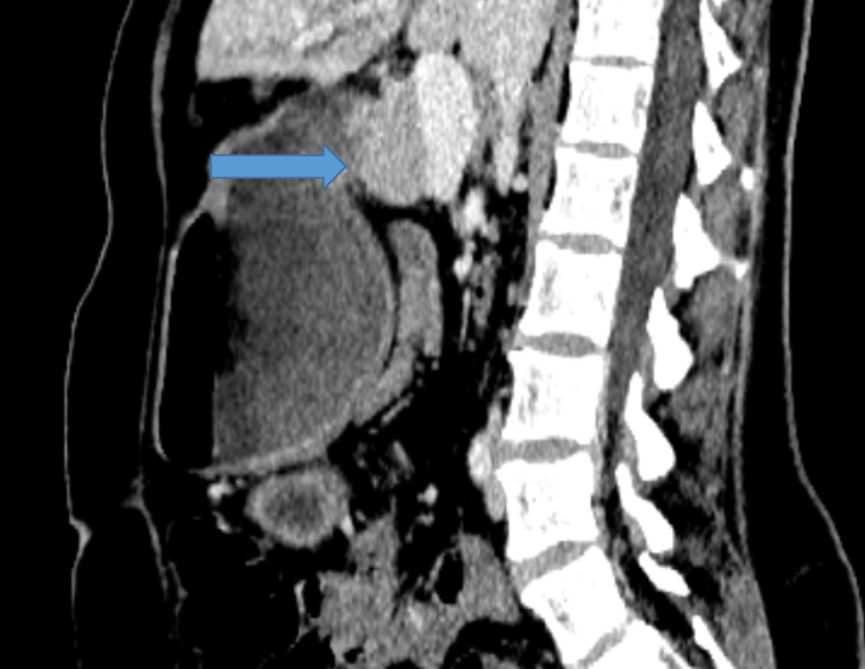
FIG 1C: Sequential sagittal sections showing pancreas partially encircling duodenum.

DIAGNOSIS
- ANNULAR PANCREAS (Incomplete type) causing gastric outlet obstruction.
DISCUSSION:
- Annular pancreas is a morphological anomaly that results in pancreatic tissue completely or incompletely encircling the duodenum.
- Can cause duodenal obstruction and is therefore important to recognize.
- Clinical presentation.
- 25% asymptomatic.
- Abdominal pain, post-prandial fullness, vomiting and gastrointestinal bleeding from peptic ulcer disease.
- Complications: pancreatitis, duodenal obstruction, rarely biliary obstruction.
- The pancreas develops from a single dorsal and two ventral buds, which appear as outgrowths of primitive foregut at 5 weeks of gestation. In the 7thweek of gestation, the duodenum expands and rotates the ventral bud from right to left which then fuses with the dorsal bud. The ventral bud forms the inferior part of uncinate process and inferior head of pancreas while the dorsal bud gives rise to the tail and body of pancreas.
- Annular pancreas develops due to failure of the ventral bud to rotate with the duodenum, causing encasement of the duodenum.
- Two types: complete/incomplete.
- Incomplete can cause significant symptoms.
- Management : surgery in symptomatic cases -> Duodenojejunostomy, gastojejunostomy

Imaging
- pancreatic tissue extending in a posterolateral direction to the second part of the duodenum in the appropriate clinical setting àraise the suspicion of annular pancreas.
- The anterolateral extension of pancreatic tissue to the second part of the duodenum is less specific for annular pancreas.
- Crocodile jaw configuration of pancreatic tissue anterior and posterior to the duodenum is highly suggestive of incomplete annular pancreas.
MRCP for evaluating ductal anatomy.

ANNULAR PANCREAS CAUSING GASTRIC OUTLET OBSTUCTION
- Approximately 33% of patients with an incomplete annular pancreas and 40% of patients with a complete annular pancreas have gastric outlet obstruction.
- Studies suggest that cause of obstruction is not entirely due to annular pancreas and underlying associated peptic ulcer disease is commonly present.
- The diagnosis of annular pancreas can be made pre-operatively by upper GI series, upper GI endoscopy, or CT scan, although 40% of diagnoses require surgery for confirmation.
REFERENCES
- Sandrasegaran K, Patel A, Fogel EL et-al. Annular pancreas in adults. AJR Am J Roentgenol. 2009;193 (2): 455-60.
- Alahmadi R. et al.: Annular pancreas: A cause of gastric outlet obstruction in a 20-year-old patient © Am J Case Rep, 2014; 15: 437-440.
Dr. Vishwanath Joshi
Consultant Radiologist.
Manipal Hospital Radiology Group (MHRG)
Manipal Hospital, Bengaluru.
Dr Anagh Vishnu
Radiology resident
Manipal Hospital, Yeshwanthpur, Bengaluru.