
39-year-old female patient who has a history of uterine fibroids came with irregular menstruation
39-year-old female patient who has a history of uterine fibroids came with irregular menstruation.
On examination:
- Abdomen is filled by a solid mass.
- Unable to feel the borders on either sides.
- Superior extent of the mass felt till epigastric region.
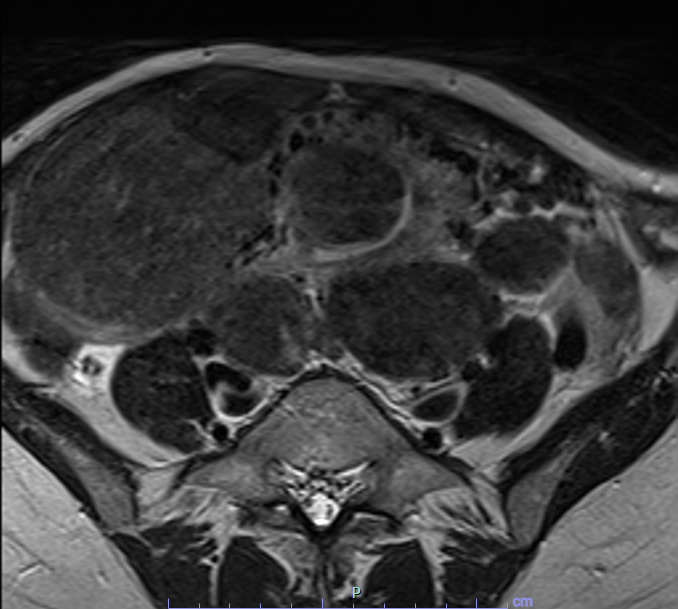
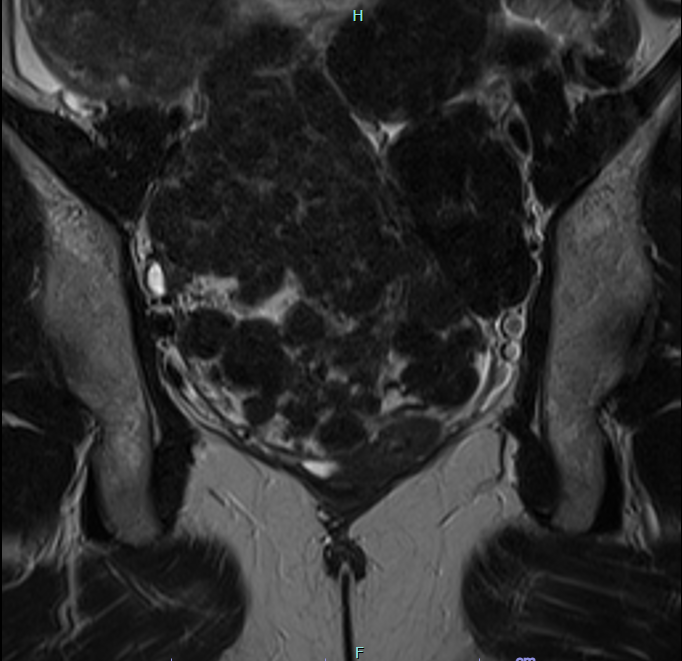
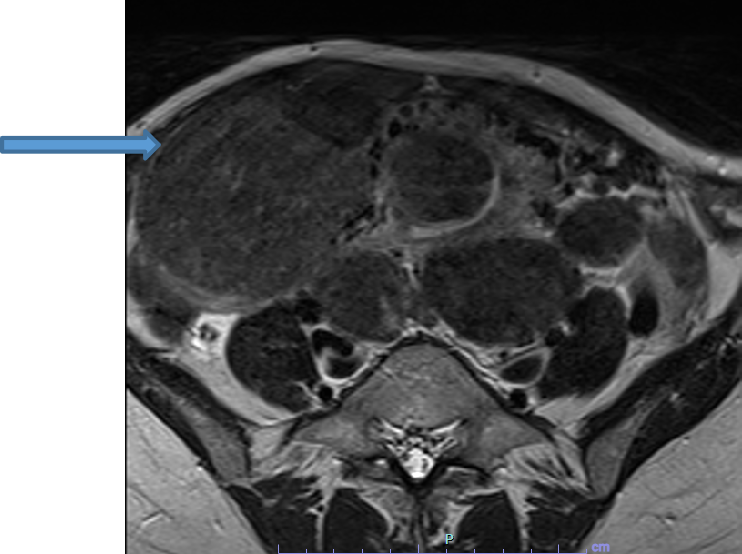
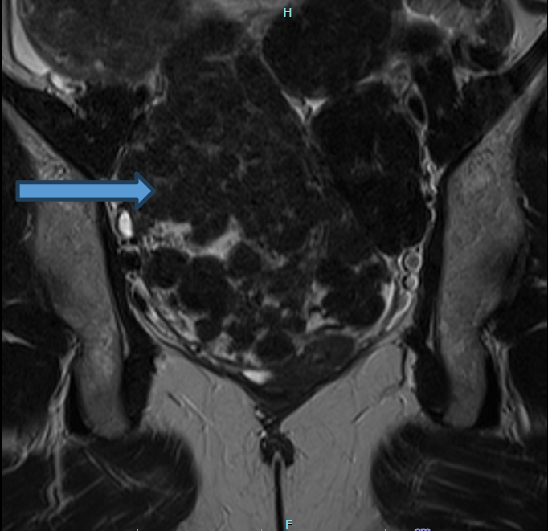
A.
- Multiple fibroids are seen filling the entire abdomen and the pelvis.
- Largest lesion in right lower quadrant is abutting the anterior abdominal wall and right psoas major with maintained fat planes.
- Largest in the left lower quadrant is abutting the left common iliac vessels and left psoas muscle.
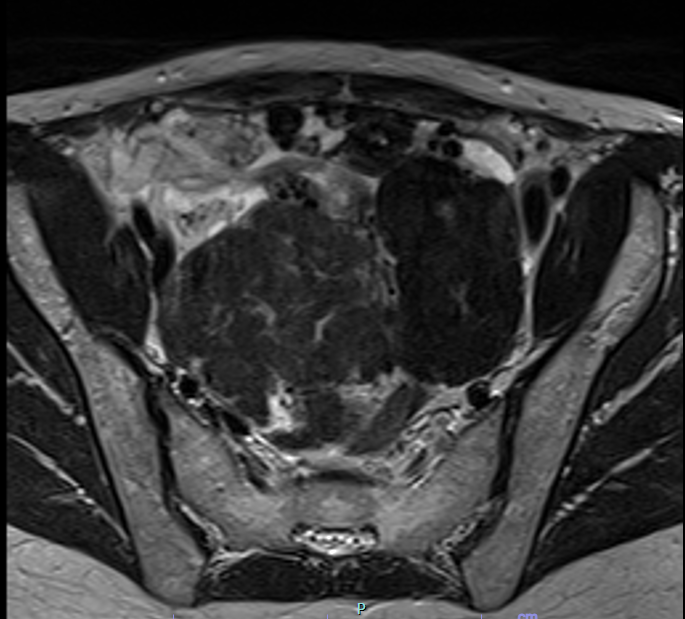
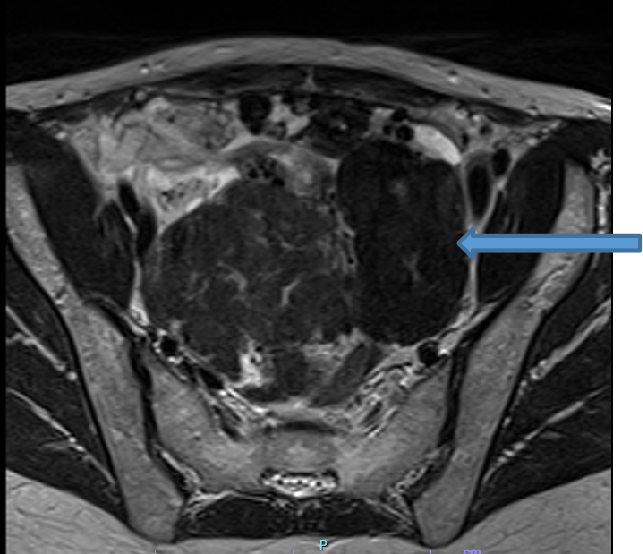
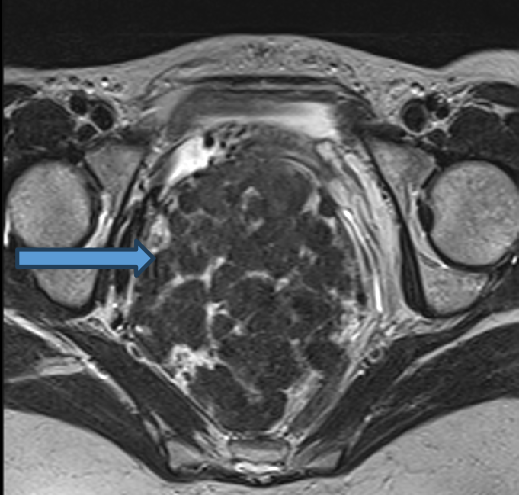
B.
- Largest lesion in the pelvis on right side is displacing the uterus anteriorly and urinary bladder antero-inferiorly.
- The recto-sigmoid courses along left lateral aspect of lesion with maintained fat planes.
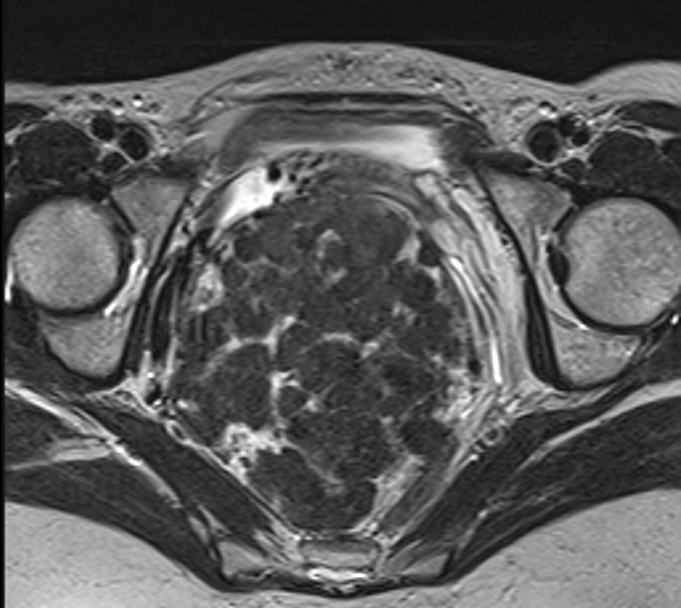
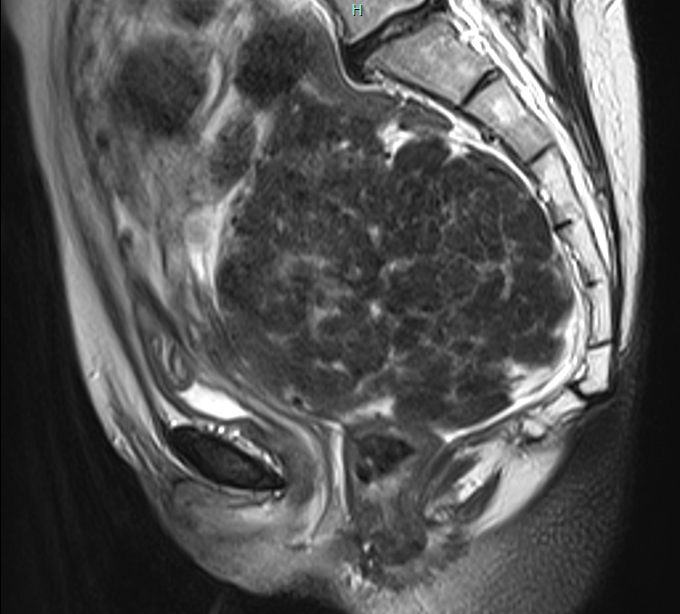
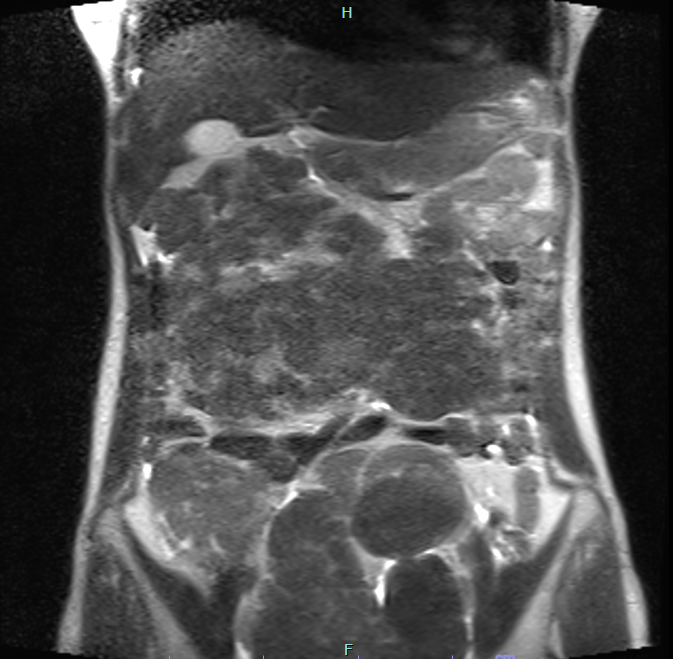
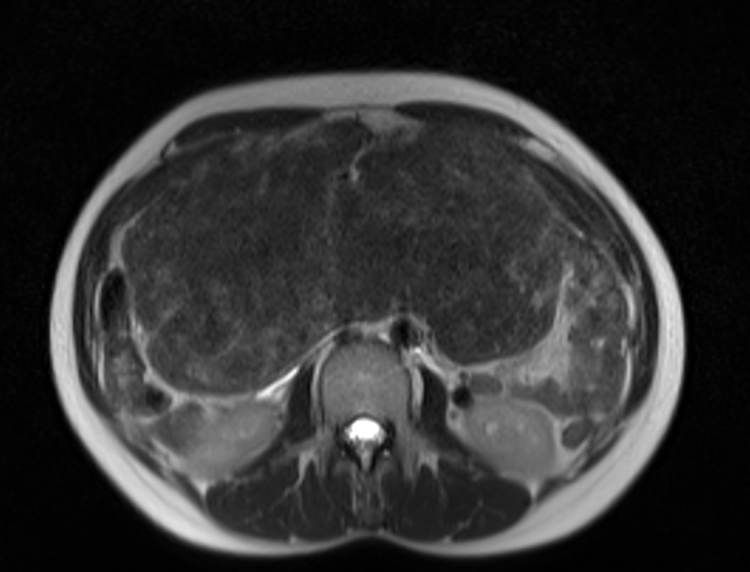
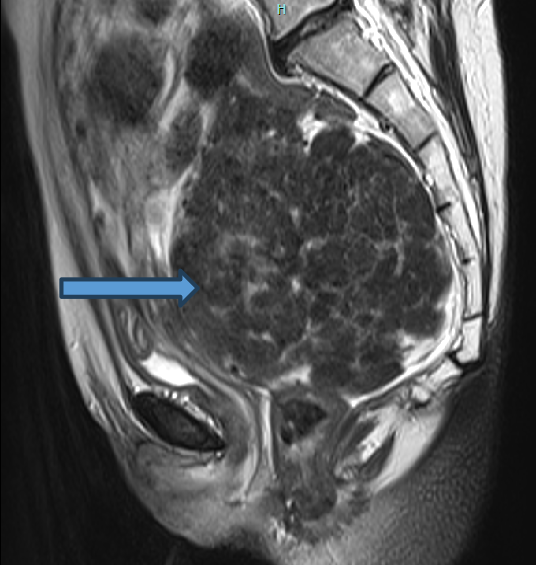
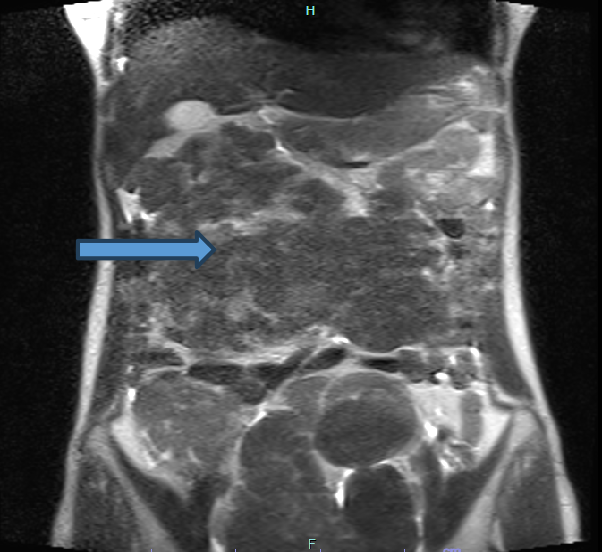
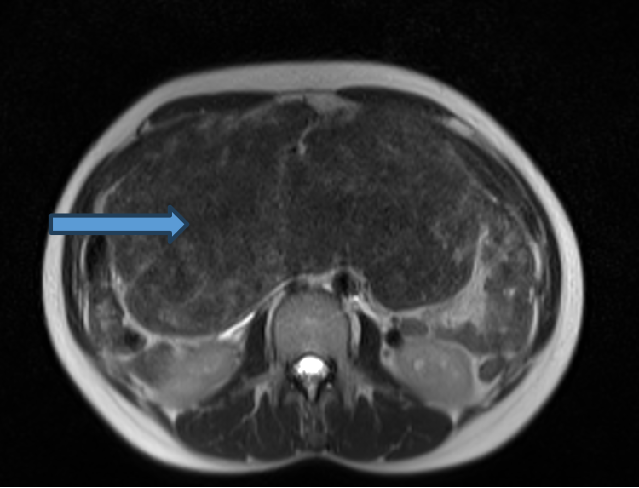
C.
- Similar morphology large abdominal lesion involving the epigastric, umbilical and right hypochondrium.
- Anteriorly the lesion is reaching up to the anterior abdominal wall with maintained fat planes.
- Posteriorly abutting the abdominal aorta and IVC with maintained fat planes.
- Superiorly the lesion is reaching up to the infrahepatic region and abutting the gallbladder with maintained fat planes. No evidence of locoregional infiltration.
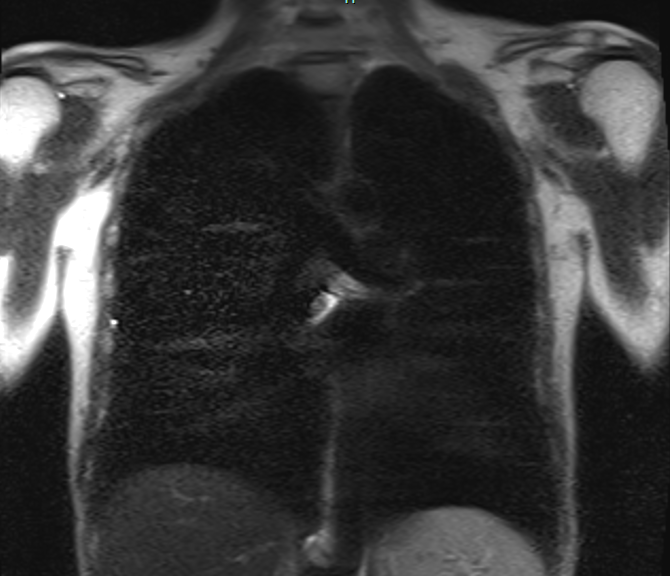
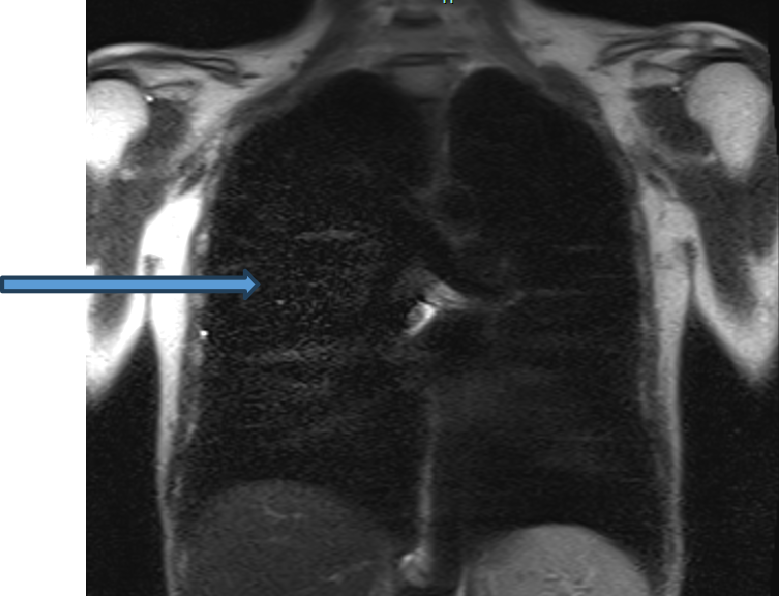
D.
- No evidence of any pulmonary metastases.
DIAGNOSIS:
- Multiple well defined heterogeneously T2 hypointense lesions in the abdomen and pelvis with associated small uterine fibroids.
- No evidence of locoregional infiltration or any aggressive features.
- Features are suggestive of diffuse peritoneal leiomyomatosis.
DISCUSSION:
- Disseminated peritoneal leiomyomatosis (DPL) is a benign rare entity characterized by the presence of innumerable smooth muscle nodules disseminated throughout the peritoneal cavity.
- This rare entity appears as multiple small nodules varying in size on or beneath the peritoneal surface, mimicking a malignancy but generally demonstrating benign histological features.
- It occurs more commonly in younger women with a history of uterine fibroids. There appears to be a relationship to hormonal factors including pregnancy, oral contraceptives, and rarely, granulosa cell tumors of the ovary.
- Laparoscopic myomectomy for treatment of uterine leiomyomas has also been implicated in the development of DPL due to dissemination of the tumor cells along the laparoscopic tract.
- The most important entity in the differential diagnosis of disseminated peritoneal leiomyomatosis is peritoneal carcinomatosis, which typically manifests with metastatic disease, weight loss, ascites, and rapid progression of disease.
- Other differential possibilities include malignant peritoneal mesothelioma, and primary peritoneal serous carcinoma.
REFERENCES
- [1] Hiremath SB, Benjamin G, Gautam AA, Panicker S, Rajan A. Disseminated peritoneal leiomyomatosis: a rare cause of enigmatic peritoneal masses. BJR Case Rep. 2016 Jul 28;2(3):20150252. doi: 10.1259/bjrcr.20150252. PMID: 30459968; PMCID: PMC6243359.
- [2] Fasih N, Shanbhogue A, Macdonald DB, Fraser-Hill MA, et al. Leimyomas beyond the Uterus: Unusual Locations, Rare Manifestations. RadioGraphics. 2008;1931-1948.
- [3] Tanaka YO, Tsunoda H, Sugano M. MR and CT findings of leiomyomatosis peritonealis disseminata with emphasis on assisted reproductive technology as a risk factor. Br J Radiol. 2009;82(975):e44-47.
Dr MADHU KUMAR
Senior Consultant Radiologist
Manipal Hospital, Yeshwanthpur, Bengaluru.
Dr PRIYANKA ROUT
Radiology resident
Manipal Hospital, Yeshwanthpur, Bengaluru.
