
38-year-old lady with complaints of sudden onset right loin to groin pain painful
HISTORY
- A 38-year-old lady with complaints of sudden onset right loin to groin pain pain.
- No history of trauma/ fever/ cough.
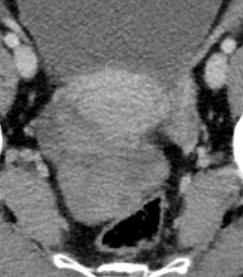

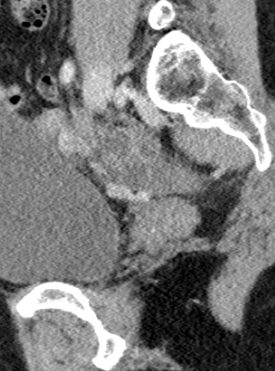
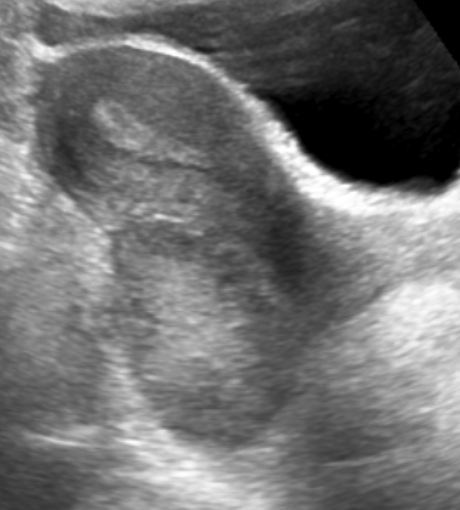
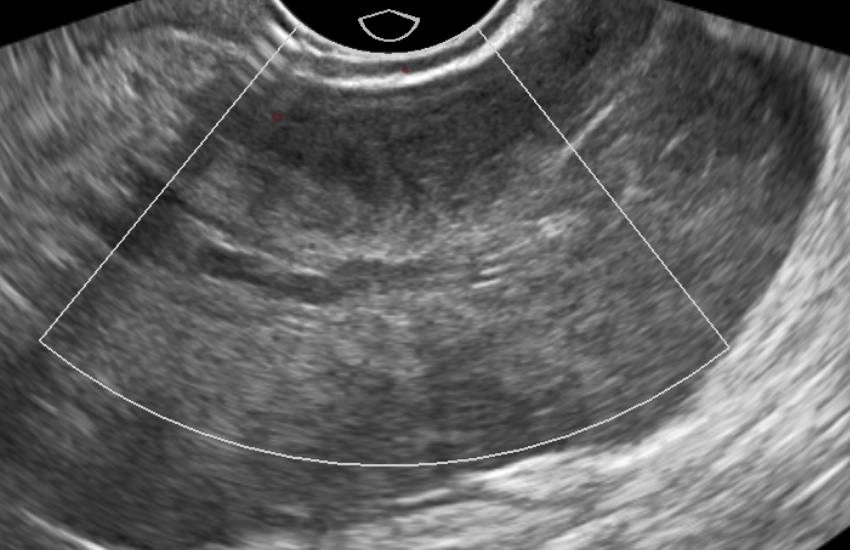
Fig 1: CECT abdomen shows enlarged heterogeneous right ovary(*) in the midline, pouch of Douglas with peripherally arranged follicles.
Fig 2 and 3: Thickened right fallopian tube with twisted appearance(black arrow).
Fig 4 and 5: USG correlates with CT finding i.e. bulky right ovary with peripherally arranged anechoic follicles(+). Color Doppler study shows no vascularity(+).
DIAGNOSIS:
- Right ovarian torsion.
DISCUSSION:
- Ovarian torsion can occur in females of all ages; however, women in their reproductive years have the highest prevalence, with 17%–20% of cases occurring in pregnant women.
- The classic presentation includes sharp, localized right or left lower abdominal pain and tenderness with a palpable abdominal mass and peritoneal signs.
- Pathophysiology: Initially, the twisted vascular pedicle in the suspensory ligament of the affected ovary compromises venous & lymphatic outflow. This results in diffuse ovarian edema and enlargement, which over time cause the capsule to stretch and increase pressure on the ovary. Arterial thrombosis and ultimately ischemia and infarction ensue. With incomplete torsion, capillary hydrostatic pressure remains increased and obstructs lymphatic drainage, causing massive ovarian edema.
- Predisposing conditions: Large, heavy cysts and cystic neoplasms, such as benign mature cystic teratomas, hemorrhagic cysts, and cystadenomas, commonly predispose the ovary to swing on its vascular pedicle. Torsion of a normal ovary is unusual but is more common in adolescents.
IMAGING FEATURES:
- US is the primary mode of evaluation of a young female patient with lower abdominal pain because it is noninvasive, acessible, and cost-effective with accurate results.
- The most constant finding in ovarian torsion is a large ovary(>4cm). The volume of the twisted ovary averages 28 times the normal size.
- The ovarian stroma may be heterogeneous due to hemorrhage and edema.
- In up to 74% of cases, US may demonstrate multiple small (up to 25 mm), uniform cysts aligned in the periphery o.f the engorged ovary
- Frequently, in up to 73% of cases, there is a complex adnexal or pelvoabdominal mass, which can be predominantly cystic, solid, or both.
- The classic color Doppler sonographic finding in ovarian torsion is the absence of arterial flow. However, the most frequent finding is either decrease or absence of venous flow.
- Promising findings incorporating both grayscale and color Doppler sonography are a twisted vascular pedicle and the whirlpool sign.
CT AND MR IMAGING
- Common findings are somewhat nonspecific and include an adnexal mass that may be in the midline, rotated toward the contralateral side of the pelvis, deviation of the uterus to the side of the affected ovary and ascites.
- Other findings include, thickened fallopian tubes, lack of enhancement, obliteration of fat planes, hematoma, and gas within the torsed mass.
MIMICS OF OVARIAN TORSION
- Common mimics of ovarian torsion are also the masses that predispose the ovary to twist on its vascular pedicle.
- Hemorrhagic ovarian cysts
- Serous cystadenomas
- Ovarian hyperstimulation syndrome
REFERENCES
- Dixon, Andrew. “Ovarian Torsion | Radiology Reference Article | Radiopaedia.Org.” Ovarian Torsion | Radiology Reference Article | Radiopaedia.Org, radiopaedia.org, https://radiopaedia.org/articles/ovarian-torsion. Accessed 4 May 2022.
- Chang, H. C., Bhatt, S., & Dogra, V. S. (2008). Pearls and pitfalls in diagnosis of ovarian torsion. RadioGraphics, 28(5), 1355–1368. https://doi.org/10.1148/rg.285075130
Dr Naveen SS, MD
Cross-sectional imaging fellow MHRG
Dr Dayanand Sagar G, MD
Consultant Radiologist MHRG.
