
31 years old, male with chronic kidney disease on dialysis, presented with headache and blurring of bilateral vision.
- 31 years old, male with chronic kidney disease on dialysis, presented with headache and blurring of bilateral vision.
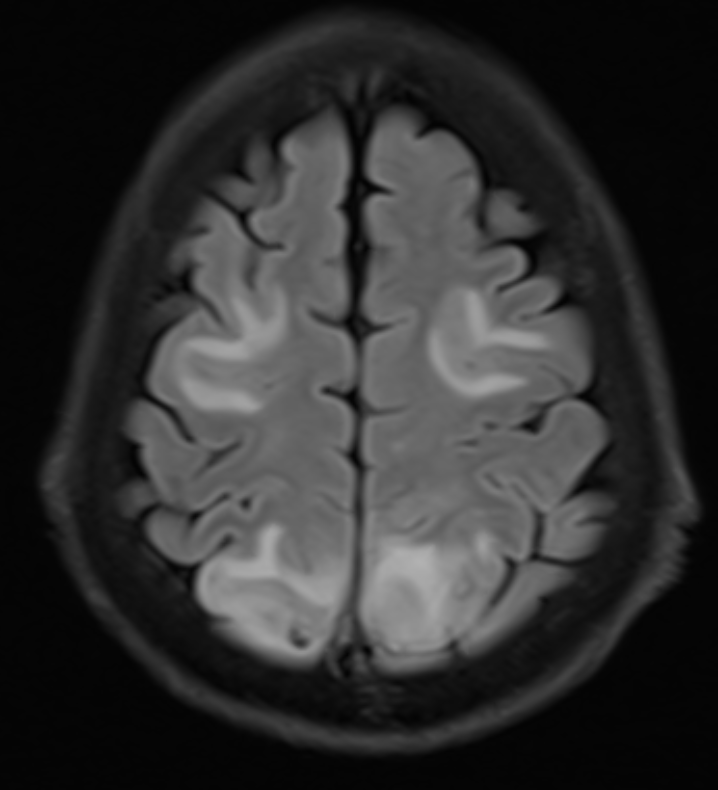
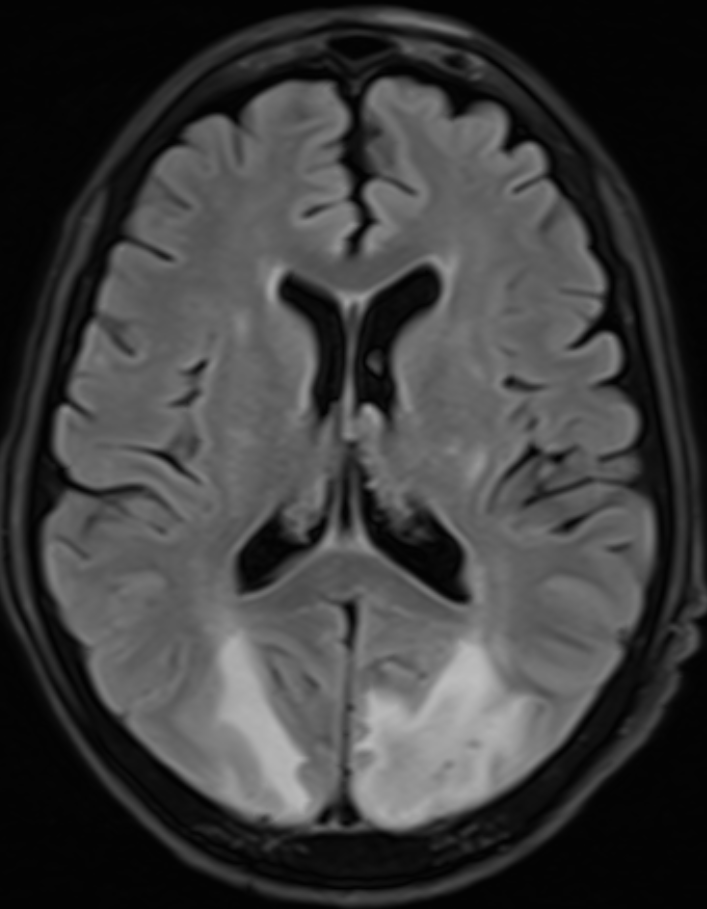
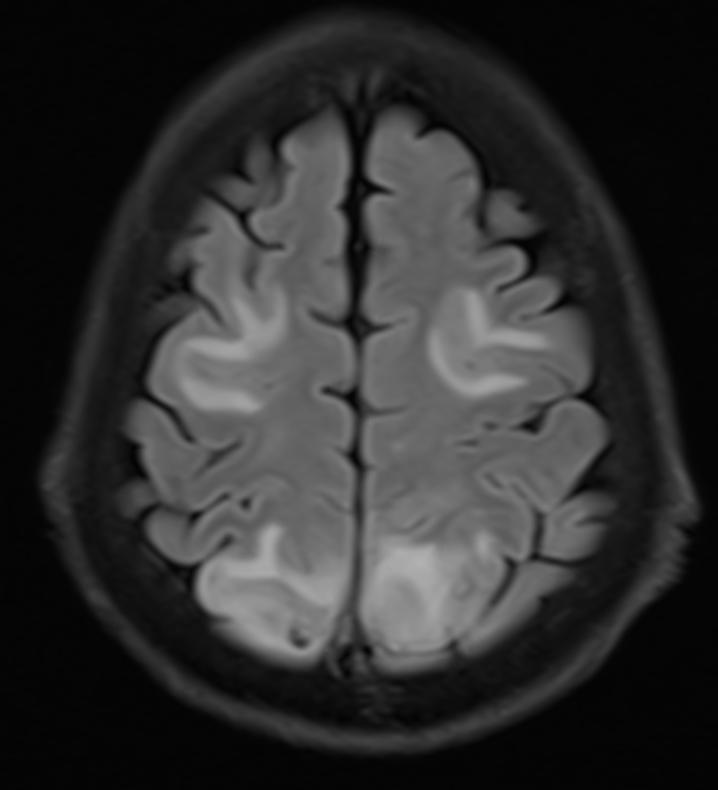
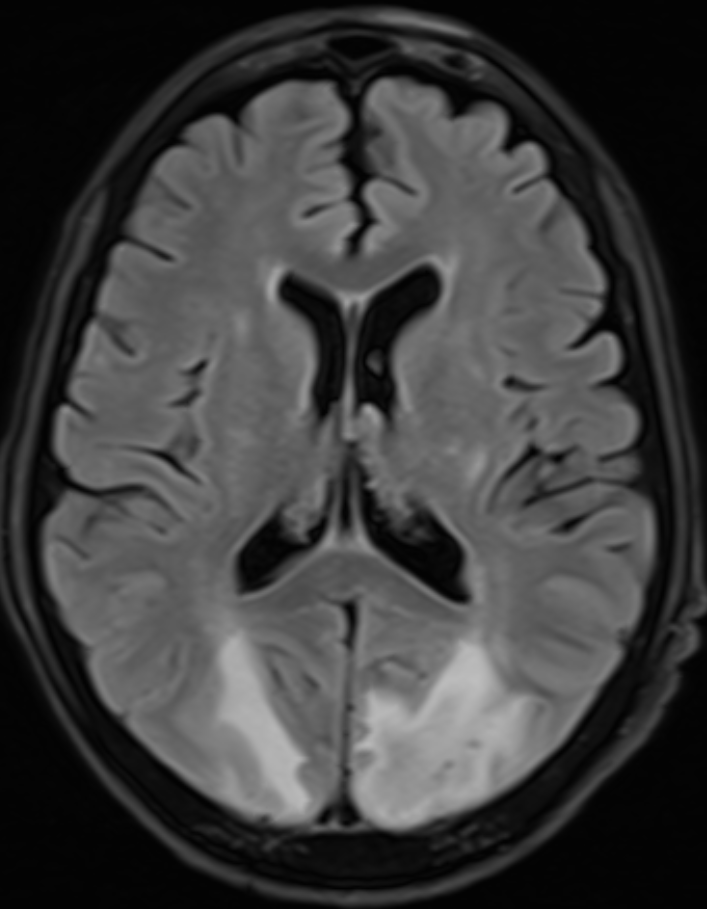
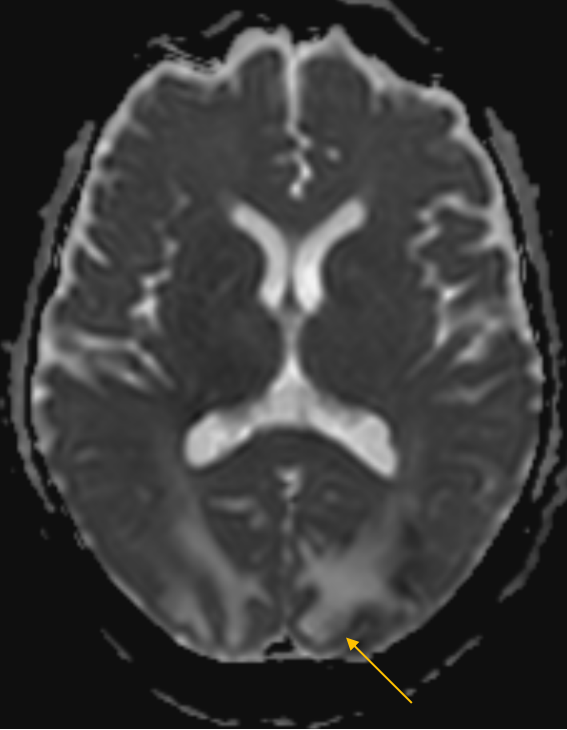
- Cortical and subcortical FLAIR hyperintensities in the bilateral frontal and parieto-occipital lobes. Subtle FLAIR hyperintensities in the bilateral basal ganglia
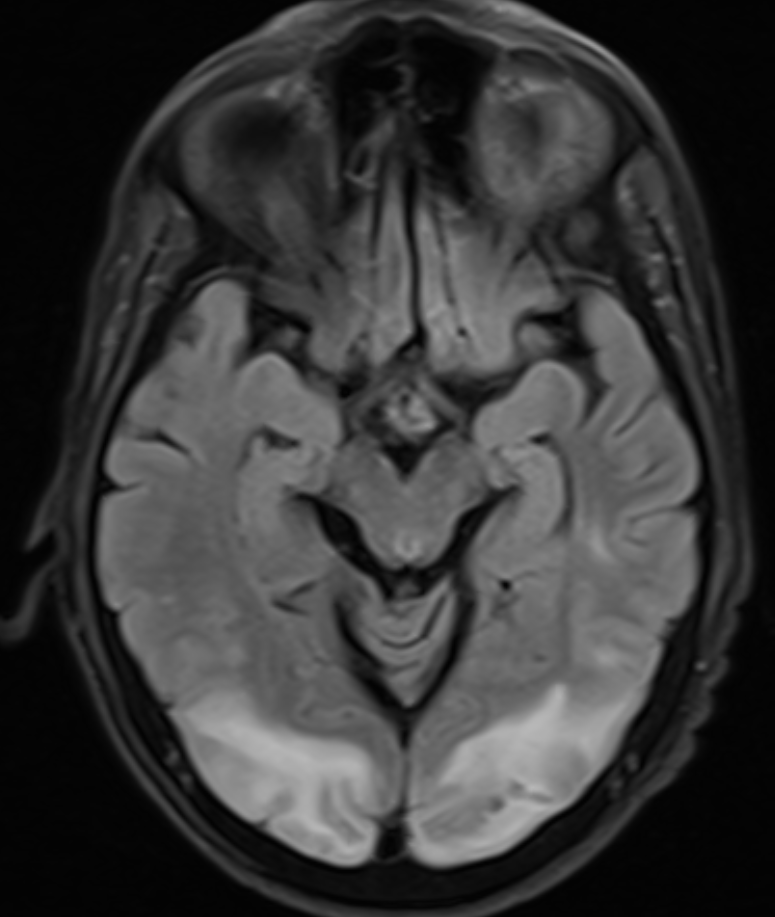
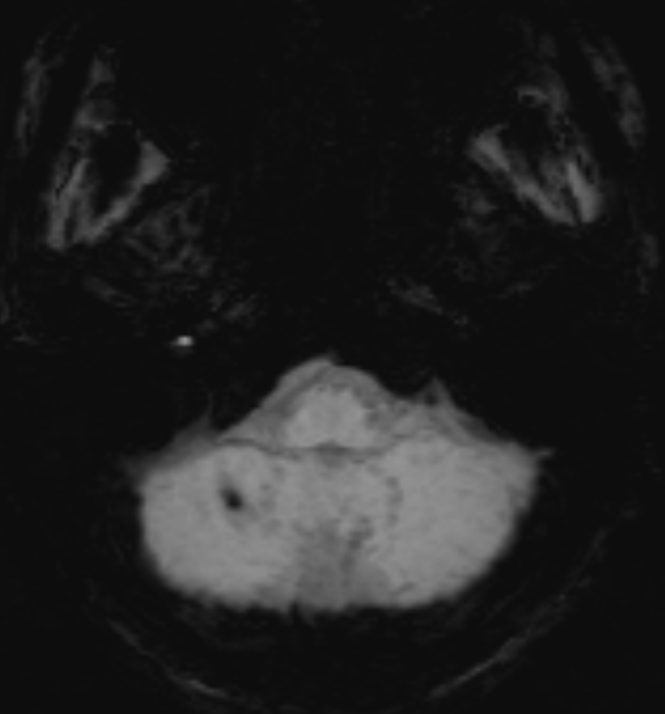
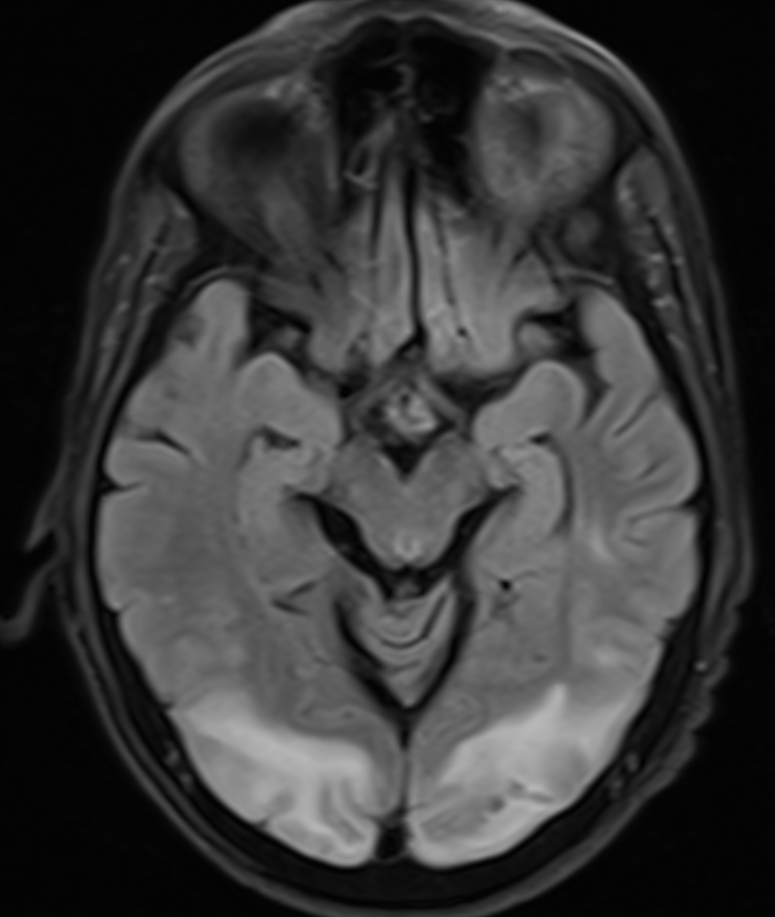
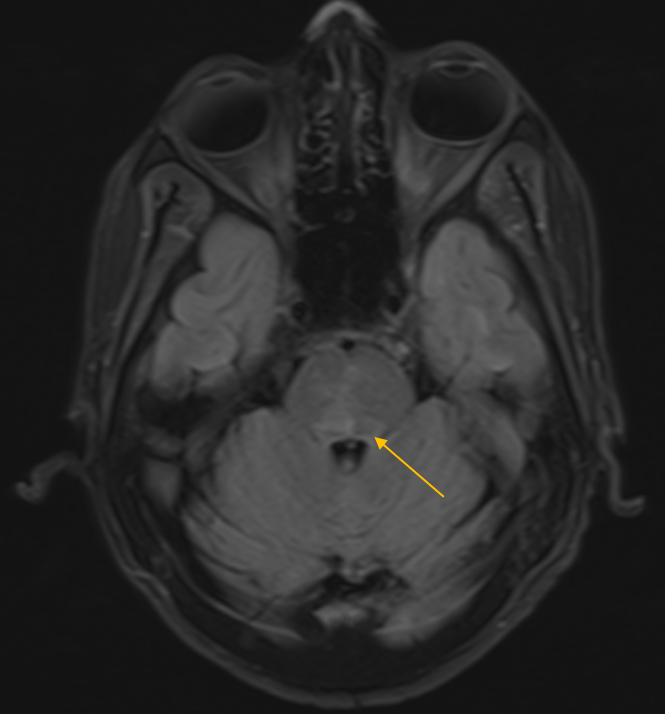
- Subtle FLAIR hyperintensities in the dorsal pons.
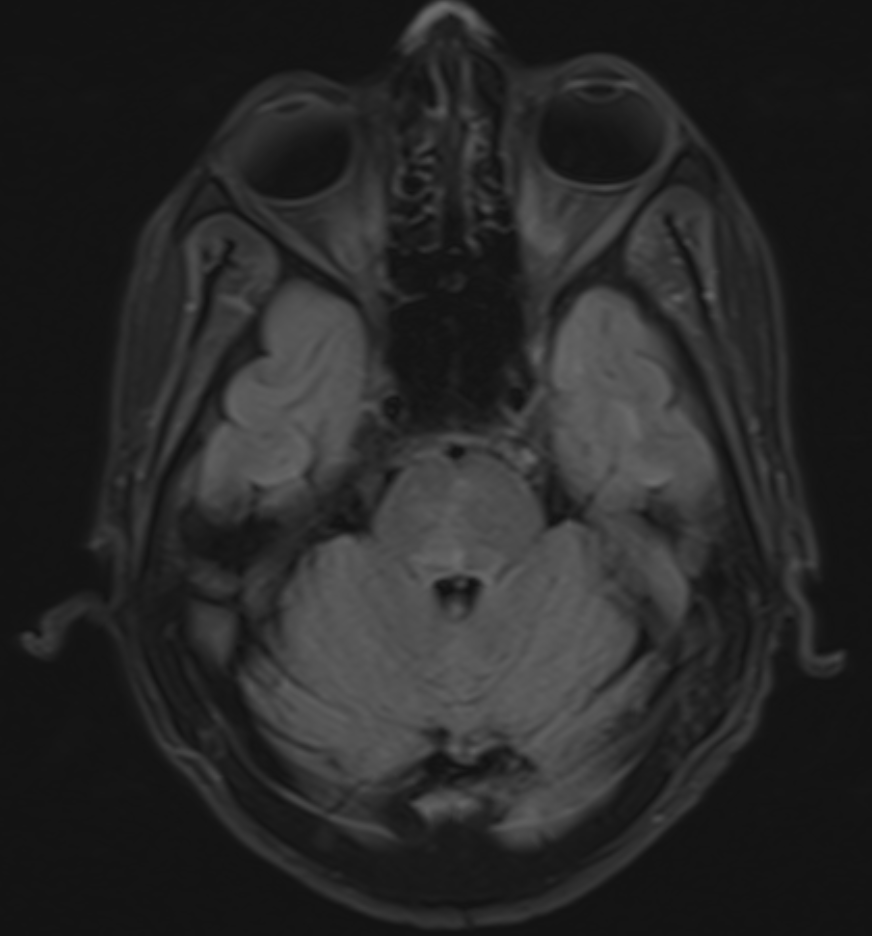
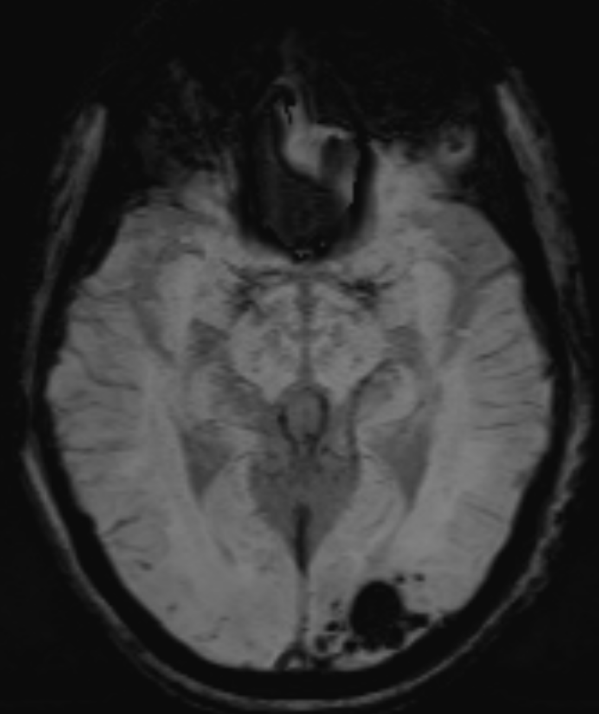
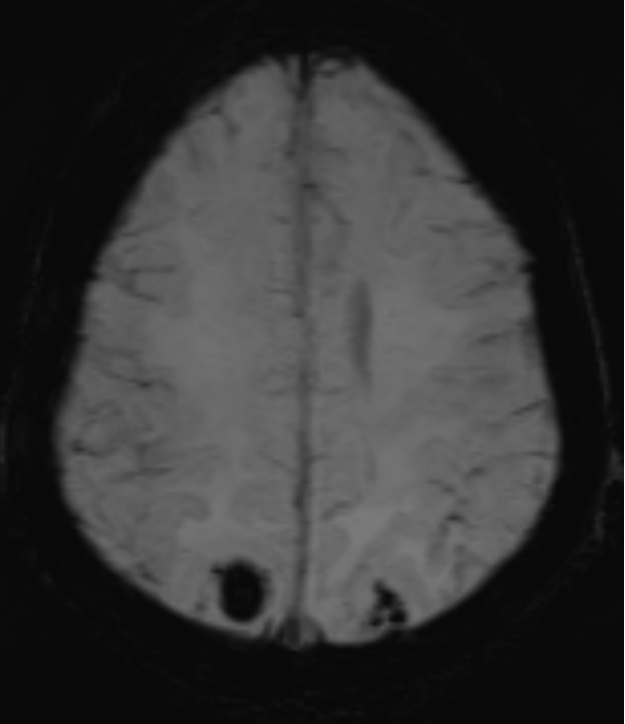
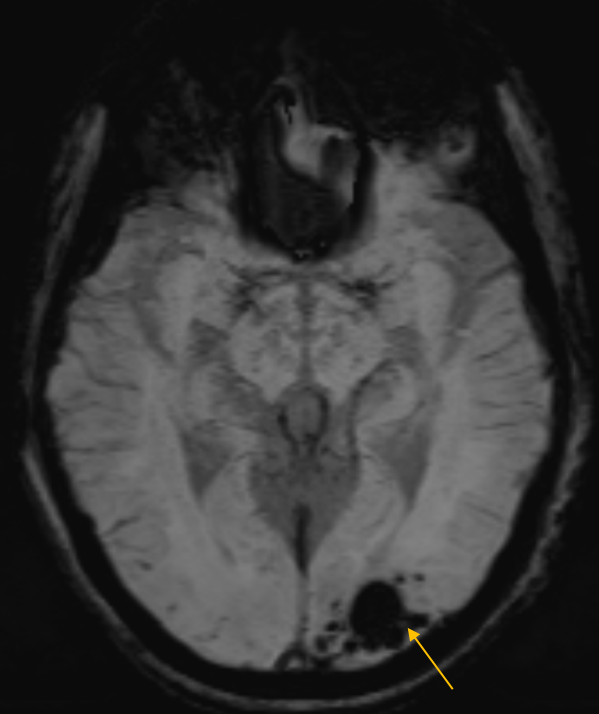
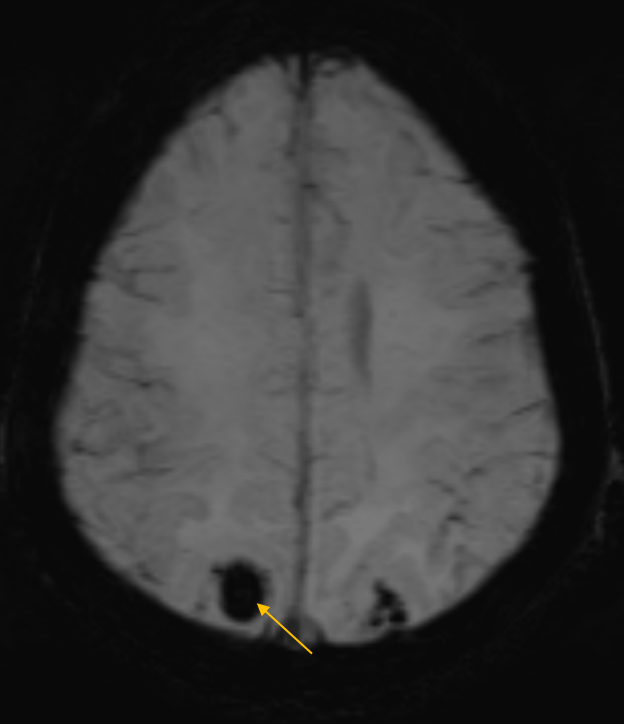
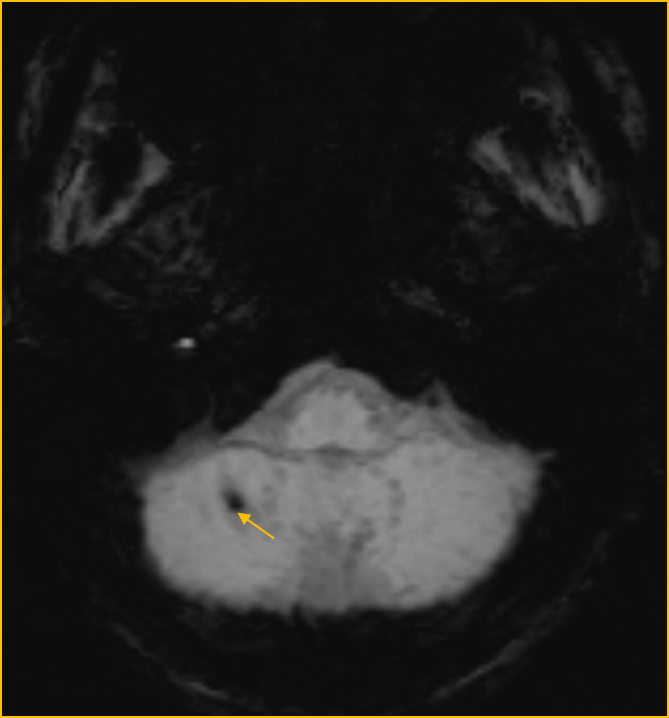
- Blooming foci within bilateral parieto-occipital lobes and right cerebellar hemisphere – suggestive of hemorrhage
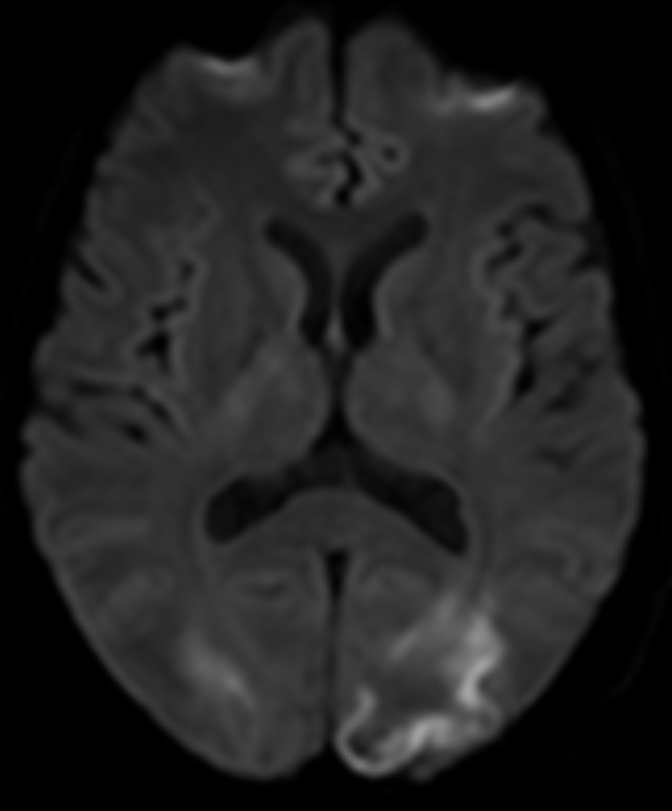
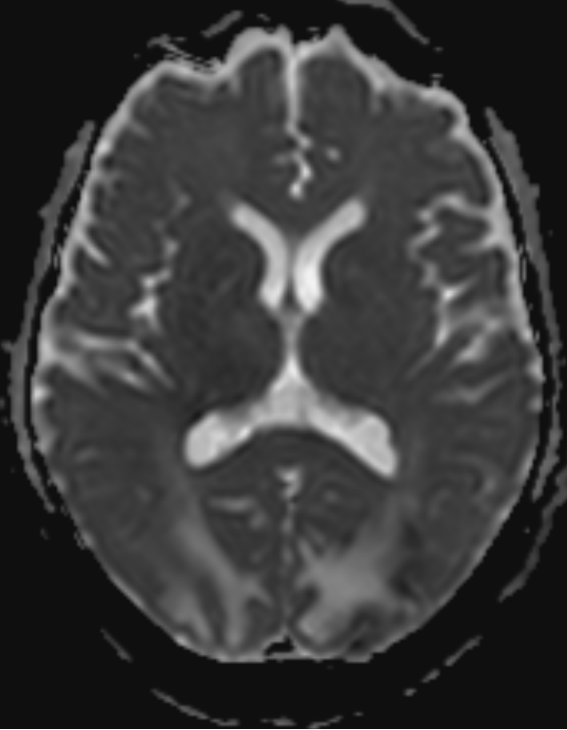
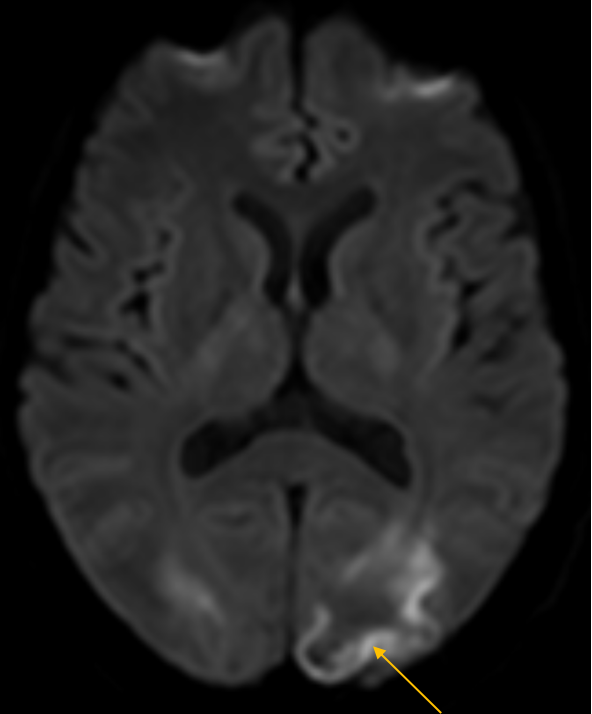
- Areas of gyral diffusion restriction in the bilateral parieto-occipital lobes.
DIAGNOSIS
- Atypical posterior reversible encephalopathy syndrome.
DISCUSSION
- Posterior reversible encephalopathy syndrome (PRES), also known as reversible posterior leukoencephalopathy syndrome (RPLS), is a neurotoxic state that occurs secondary to the inability of the posterior circulation to autoregulate in response to acute changes in blood pressure.
- Hyperperfusion with resultant disruption of the blood-brain barrier results in vasogenic edema, usually without infarction, most commonly in the parieto-occipital regions.
- Typical MRI appearance of PRES includes T2W and FLAIR hyperintensities in the parieto-occipital lobes.
Atypical presentation of PRES:
1.Involvement of atypical regions:
- Isolated involvement of deep gray nuclei
- Brainstem/cerebellar hemispheres
- Spinal cord without cerebral hemispheric involvement.
2.Hemorrhage in PRES:
- Focal petechial/microhemorrhages (<5 mm), sulcal subarachnoid hemorrhage and focal hematoma formation.
- Hemorrhage was significantly more common in patients following bone marrow transplantation than in solid organ transplantation.
3. Diffusion restriction in PRES:
- Vasogenic edema predominates in PRES, however cases may be complicated by the development of cytotoxic edema as indicated by diffusion restriction.
4. CONTRAST ENHANCEMENT IN PRES:
- Contrast enhancement has been variably reported in the setting of PRES, typically presenting as leptomeningeal or gyral cortical enhancement.
- PRES complicated by hemorrhage had a poor clinical outcome.
- Death was seen in 50% of the patients who exhibited diffusion signal changes.
- Additionally, brainstem involvement by PRES is associated with a poorer outcome.
Differential Diagnosis:
- Inflammatory cerebral amyloid angiopathy
- Severe hypoglycemia
- Posterior circulation infarct
- Hypertensive brainstem encephalopathy
- Sagittal sinus thrombosis
- Hypoxic-ischemic encephalopathy
- SMART syndrome
References
- Saad AF, Chaudhari R, Wintermark M. Imaging of atypical and complicated posterior reversible encephalopathy syndrome. Frontiers in neurology. 2019 Sep 4;10:964.
- Aracki-Trenki? A, Stojanov D, Trenki? M, Radovanovi? Z, Ignjatovi? J, Risti? S, Trenki?-Bozinovi? M. Atypical presentation of posterior reversible encephalopathy syndrome: clinical and radiological characteristics in eclamptic patients. Bosnian journal of basic medical sciences. 2016 Aug;16(3):180.
Dr Harsha Chadaga
Senior Consultant and Head of Radiology
Manipal Hospital, Yeshwanthpur Bengaluru
Dr Rashmi Jayakar Poojary
Radiology Resident
Manipal Hospital, Yeshwanthpur Bengaluru