
30 year old presented with complaints of abdominal pain , nausea with fever and hematemesis for 2 days
30 The 30-year-old presented with complaints of abdominal pain, nausea with fever, and hematemesis for 2 days
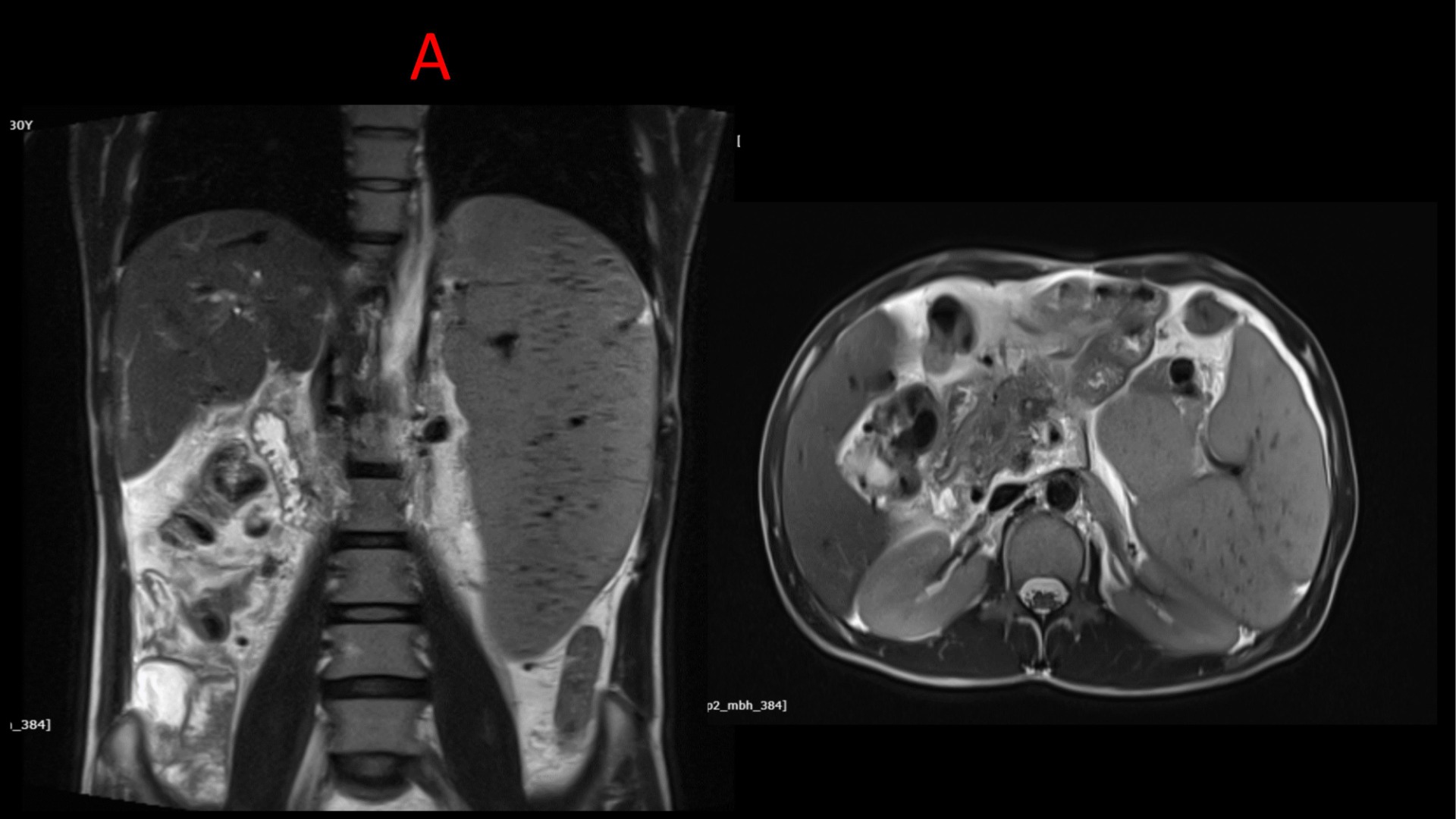
A : T2 weighted images shows massive splenomegaly with multiple tiny hypodense nodules (siderotic nodules)
Multiple dilated collaterals at porta replacing the portal vein
Liver normal signal intensity with enlarged caudate lobe and volume redistribution without any nodularity.
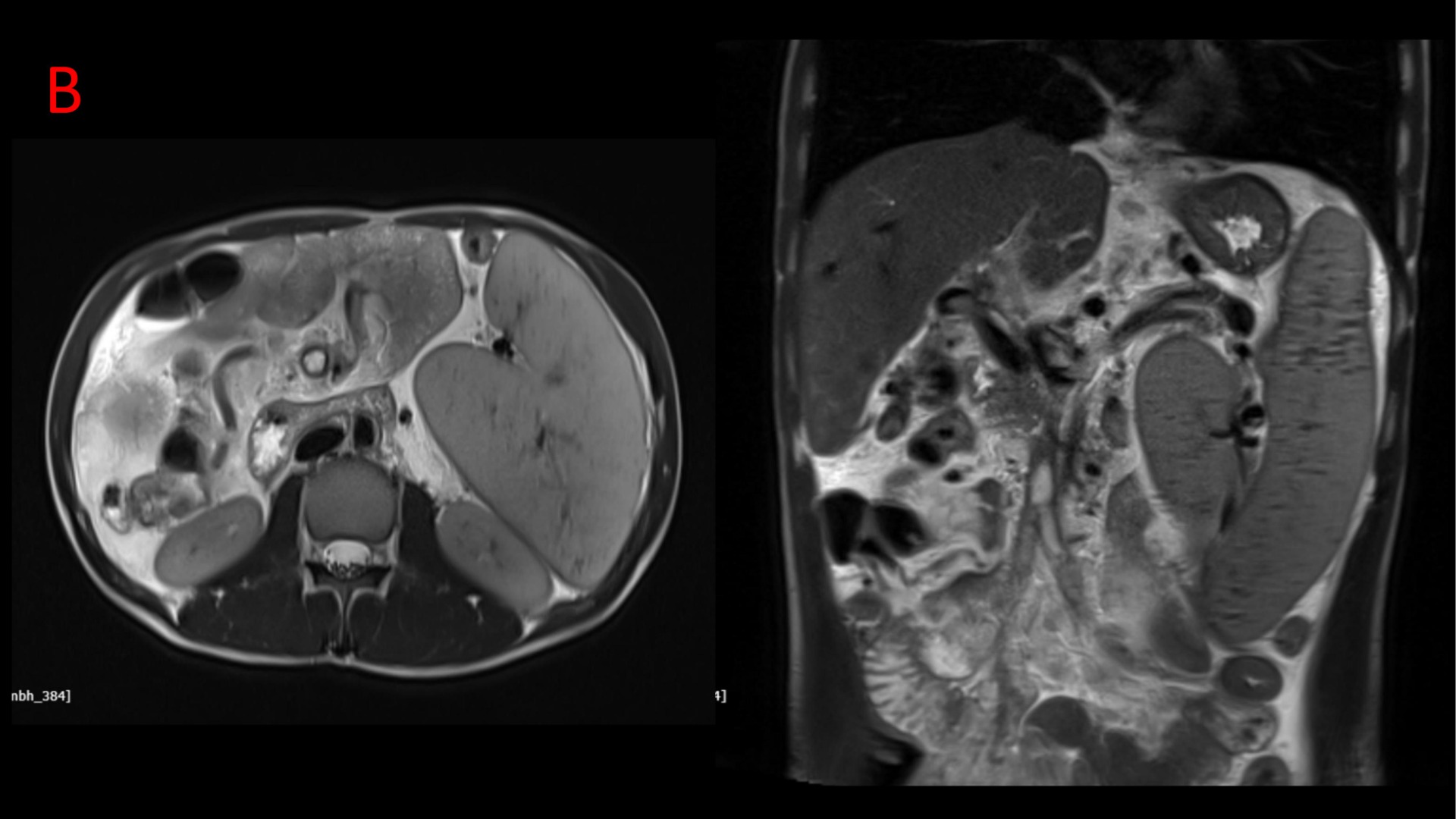
B : T2 weighted images showing dilated superior mesenteric vein with loss of T2 flow void
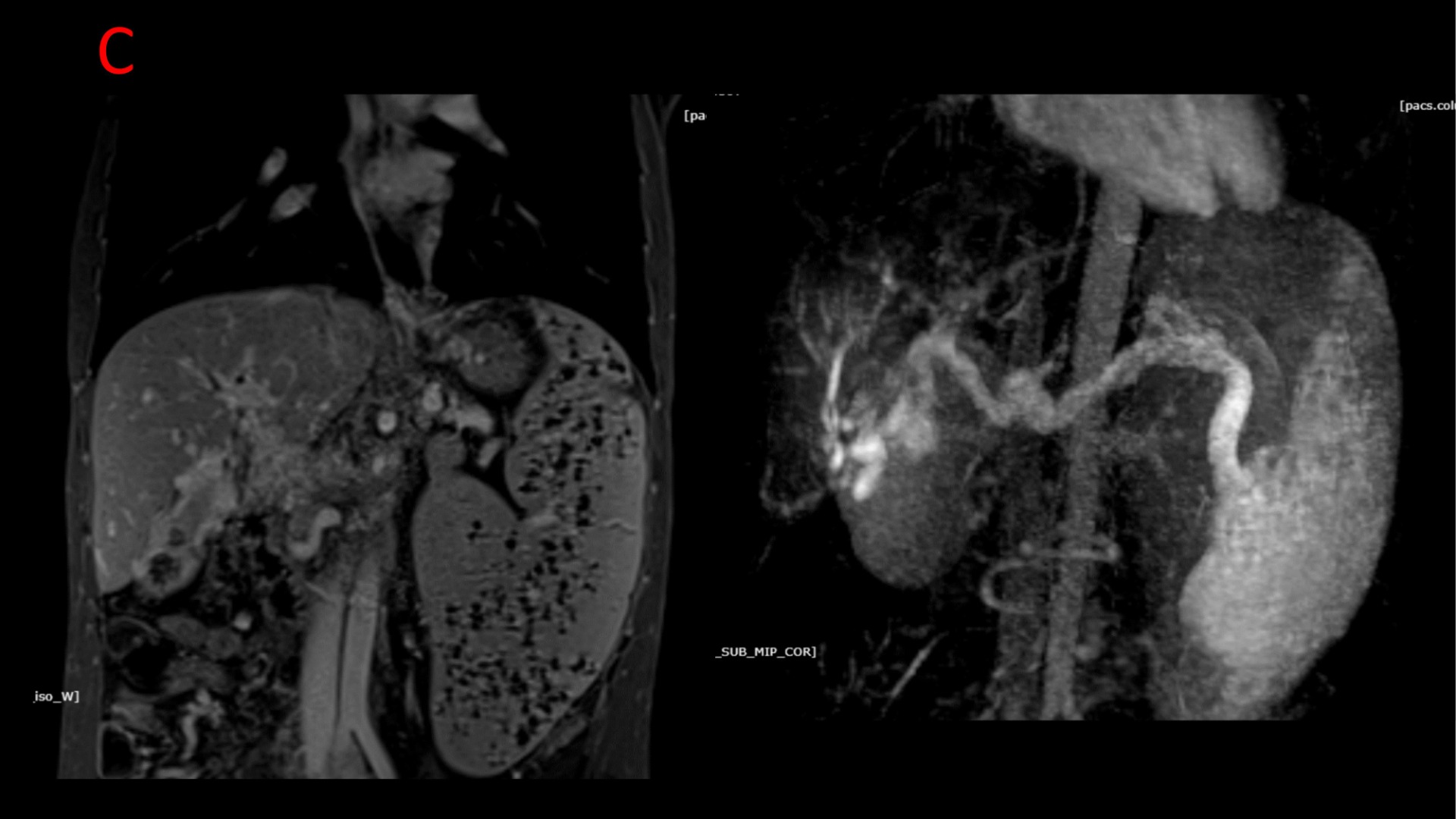
C : MR Porto-venography shows loss of flow in superior mesenteric vein with multiple dilated and tortuous epicholedocal, pericholedocal and pericholecystic collaterals. Portal vein is replaced by multiple collaterals leading to portal cavernoma formation.
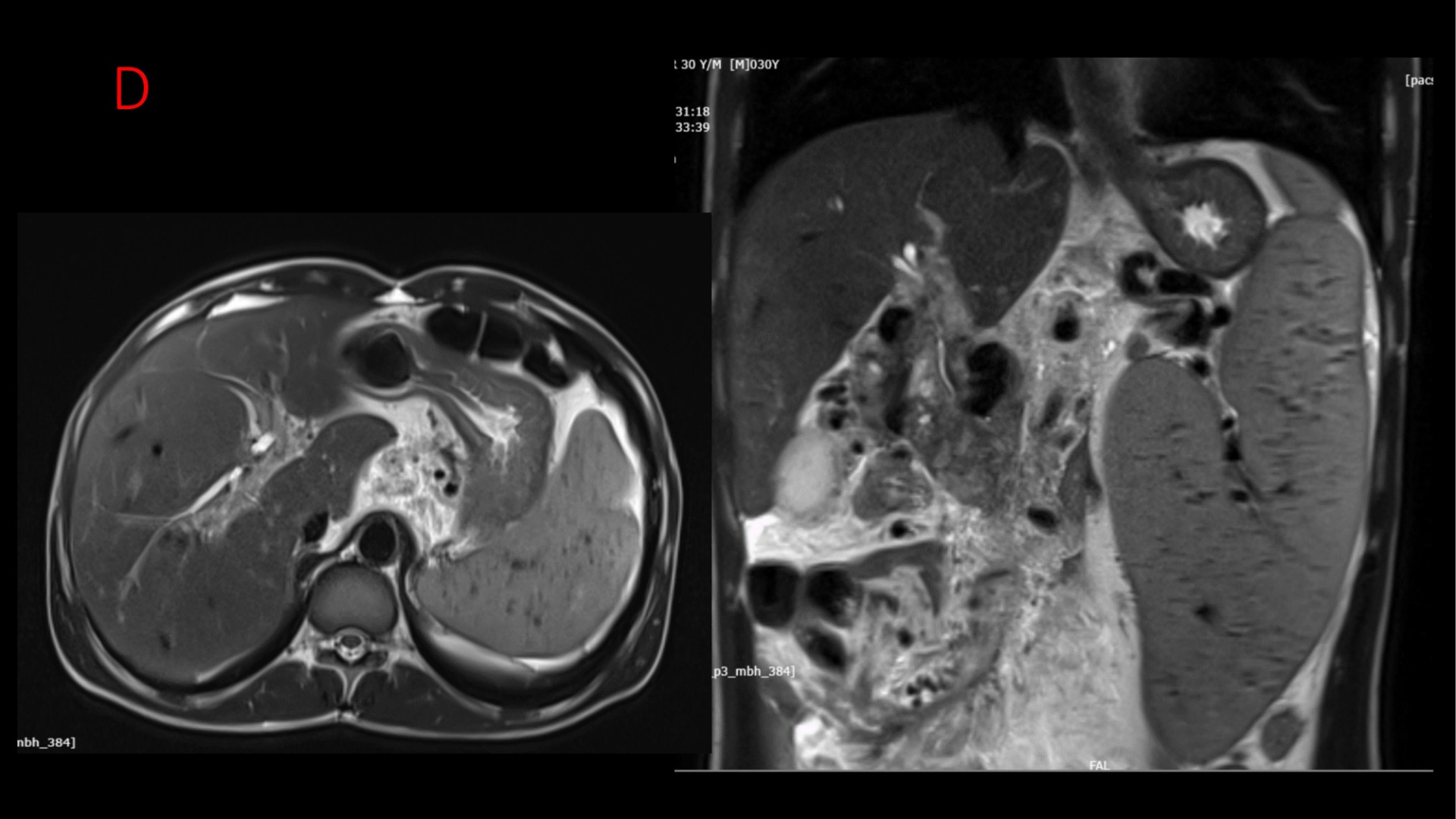
D : The collaterals are seen encasing the suprapancreatic common bile duct, CHD, left and right hepatic ducts. The common bile duct shows mildly reduced calibre with mild prominence of central intra hepatic biliary radicles.
Extrahepatic portal venous obstruction with portal cavernoma, multiple portosystemic collaterals, SMV thrombosis with massive splenomegaly and portal biliopathy.
Discussion:
- Extrahepatic portal vein obstruction is the most common cause of non-cirrhotic portal hypertension in children and young adults in developing countries.
- It may or may not extend into the intrahepatic portal vein.
Clinical presentation:
It usually occurs in children and young adults, presenting as unexplained gastrointestinal bleeding.
Other features include:
- Obstructive jaundice may be seen due to extrahepatic compression of the bile ducts by cavernous collaterals.
- Splenomegaly.
- Ascites.
Etiology:
- Idiopathic (50% cases)
- Children:
- neonatal infections
- Umbilical vein catheterisation
- developmental anomalies
- trauma/surgery
- Young adults:
- infections
- neoplastic diseases
- Pancreatitis
- myeloproliferative disorders
- hypercoagulable states
Imaging features:
- Extrahepatic portal vein obstruction (EHPVO) is characterized by features of recent thrombosis or portal hypertension with portal cavernoma as a sequel of portal vein obstruction.
- Imaging of spleno-portal axis is the mainstay for the diagnosis of EHPVO.
Imaging features include:
- Normal liver echotexture.
- Splenomegaly.
- Collaterals along spleno-portal axis.
- Cavernous transformation of portal vein.
- Ascites.
Radiologic Assessment
- Includes imaging of the main portal vein, its right and left branches, splenic vein, and superior mesenteric vein, evidence of portal biliopathy, status of collaterals, and possible sites for portosystemic shunt surgery.
- Color Doppler ultrasound is the first imaging modality used and is accurate in the assessment of the portal venous system.
- However in patients who are potential candidates for portosystemic shunt procedures, MDCT and MR portovenography play an indispensable role in identifying portal vein thrombosis, abdominal collaterals and visceral changes.
Treatment
Options include:
- Endoscopic variceal band ligation.
- Endoscopic sclerotherapy.
- Rex shunt: mesentrico-left portal vein shunt.
- Rex segment (umbilical segment of the left portal vein) must be patent for this
- retrograde portography may be used to identify its patency if non-invasive imaging fails
- Splenorenal shunt (distal or proximal).
Conclusion
- Extrahepatic portal vein obstructionis the most common cause of non-cirrhotic portal hypertension in children and young adults.
- Clinically presents with unexplained bleeding and obstructive jaundice.
- Imaging plays an indispensable role in diagnosis of EHPVO.
- Though USG and MRI are complementary to each other in pre operative assessment of portal venous system, MR porto-venography is more sensitive and superior to color Doppler and also has the added advantage of delineating changes in intrahepatic biliary ducts.
References
- Sarin SK, Sollano JD, Chawla YK et-al. Consensus on extra-hepatic portal vein obstruction. Liver Int. 2006;26 (5): 512-9. doi:10.1111/j.1478-3231.2006.01269.x– Pubmed citation
- Poddar U, Borkar V. Management of extra hepatic portal venous obstruction (EHPVO): current strategies. Trop Gastroenterol. 2011;32 (2): 94-102. Pubmed citation
- 3. Sharma MP, Dasarathy S, Misra SC et-al. Sonographic signs in portal hypertension: a multivariate analysis. Trop Gastroenterol. 1996;17 (2): 23-9. Pubmed citation
Dr. Sharnitha Johnson
Cross-sectional Fellow
Manipal Hospital Radiology Group (MHRG)
Manipal Hospital, Bengaluru
Dr. Vishwanath Joshi
Consultant Radiologist.
Manipal Hospital Radiology Group (MHRG)
Manipal Hospital, Bengaluru.

