30-year-old female, presented with severe right lower abdominal pain, since 1 day
-
30-year-old female, presented with severe right lower abdominal pain, since 1 day
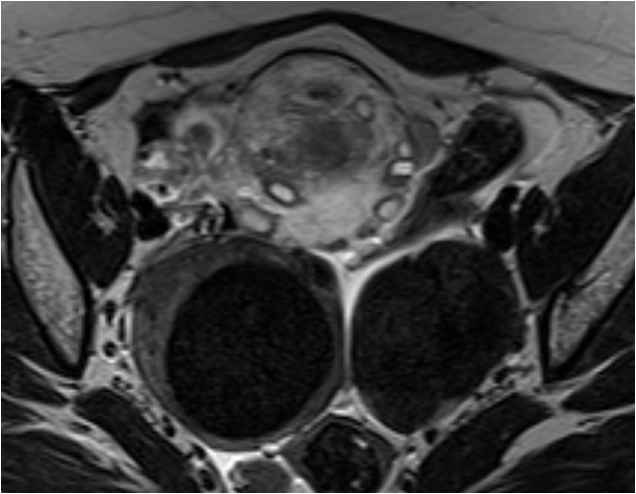
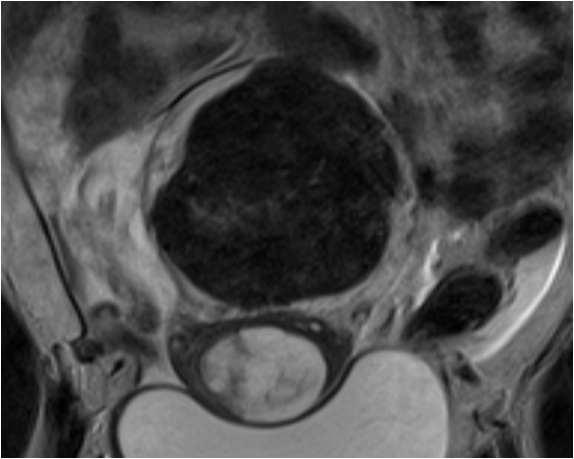

- Enlarged T2 hyperintense /edematous right ovary located in the midline pelvis showing peripherally displaced follicles.
- Thickened right ovarian pedicle with apparent whirled appearance.
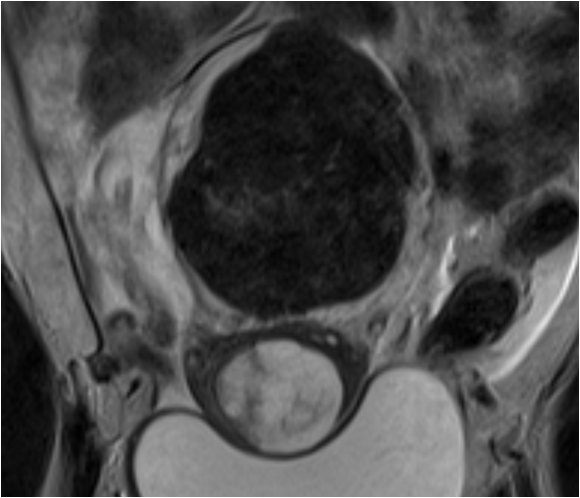
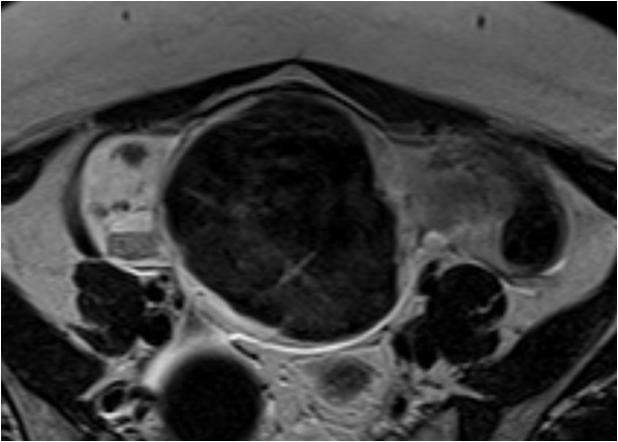
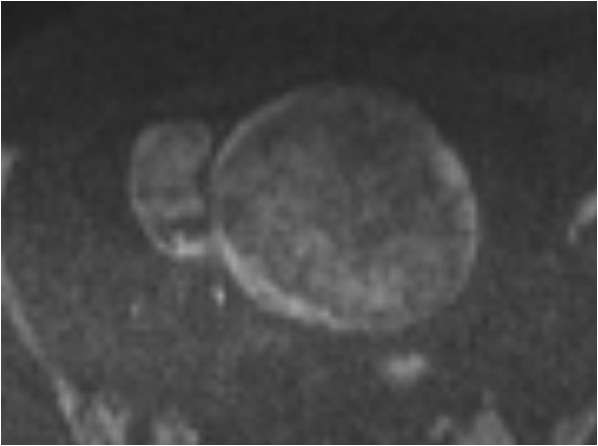
Mild free fluid in the pelvis. - A T2 hypointense, non-diffusion restricting, solid lesion in the right ovary.
- A similar T2 hypointense lesion was also found in the left ovary.

Diagnosis:
- Bilateral ovarian fibroma with ovarian torsion.
- Histopathological evaluation, after laparoscopic oophorectomy, confirmed diagnosis of Brenner’s tumor.
Discussion:
- Ovarian torsion – rotation of the ovary and portion of the fallopian tube supplying the vascular pedicle.
- Torsion occurs due to two main reasons:

- Most lesions are dermoid cysts or paraovarian cysts.
- Large cystic ovaries undergoing ovarian hyperstimulation are at particular risk.
- Masses between 5-10 cm are at most risk
Pointers to ovarian torsion on CT and MRI:
- Enlarged ovary
- Involved ovary shifted to the midline and most often anterior to the uterus
- Lead mass may be identified
- Twisted pedicle in the adnexa
- Uterus displaced to the involved side
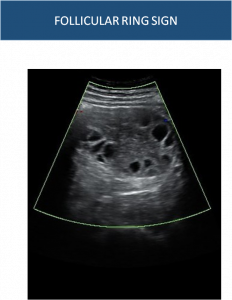
- Characteristic sonographic sign for early diagnosis of ovarian torsion.
- A prominent (1-2 mm thick) hyperechoic margin seen concentrically around the antral follicles of the torsed ovary, which are usually small and peripherally displaced.
Brenner tumor
- Uncommon surface epithelial tumor of the ovary.
- MRI: Homogeneous isointensity to the uterine muscle on T1 and markedly low signal intensity on T2 images. Patchy mild post contrst enhancement may be noted.
Brenner vs Fibroma:
Brenner tumours are predominantly homogenous, unlike the usual appearance of larger fibromas, which usually show internal edema and cystic change in larger lesions. Although the two tumors are not likely to be differentiable by MR imaging.
REFERENCE:
- Chiou SY, Lev-Toaff AS, Masuda E, Feld RI, Bergin D. Adnexal torsion: new clinical and imaging observations by sonography, computed tomography, and magnetic resonance imaging. Journal of Ultrasound in Medicine. 2007 Oct;26(10):1289-301.
- Sibal M. Follicular ring sign: a simple sonographic sign for early diagnosis of ovarian torsion. Journal of ultrasound in medicine. 2012 Nov;31(11):1803-9.
- Outwater EK, Siegelman ES, Kim B, Chiowanich P, Blasbalg R, Kilger A. Ovarian Brenner tumors: MR imaging characteristics. Magnetic resonance imaging. 1998 Dec 1;16(10):1147-53.
Dr. Vikhyath Shetty
Consultant Radiologist
Manipal Hospital, Yeshwanthpur.
Dr Rashmi Jayakar Poojary
Primary DNB Radiology Resident
Manipal Hospital Yeshwanthpur.