
3 year old male patient with swelling over the head from birth, gradually increasing in size since the last 3 months.Normal growth and developmental milestones
3 year old male patient with swelling over the head from birth, gradually increasing in size since the last 3 months.Normal growth and developmental milestones.
On examination:
- Well alert, playful
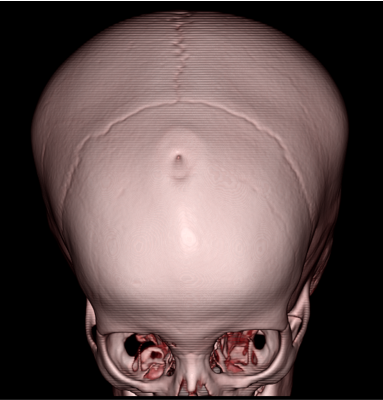
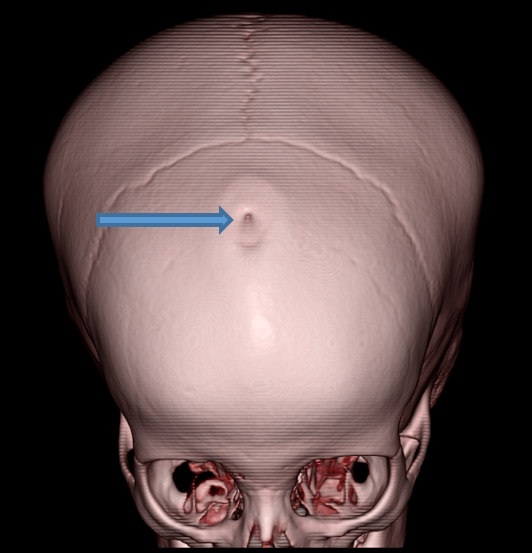
- A swelling of size approximately 2cm noted over the fontanelle
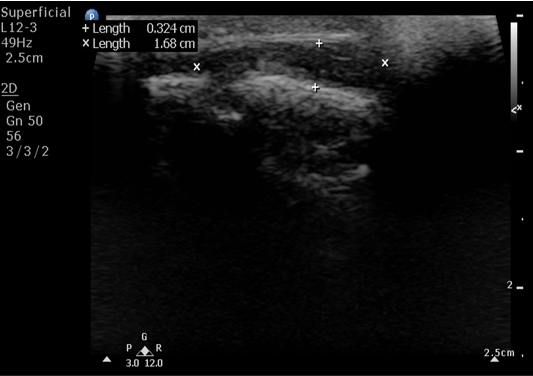
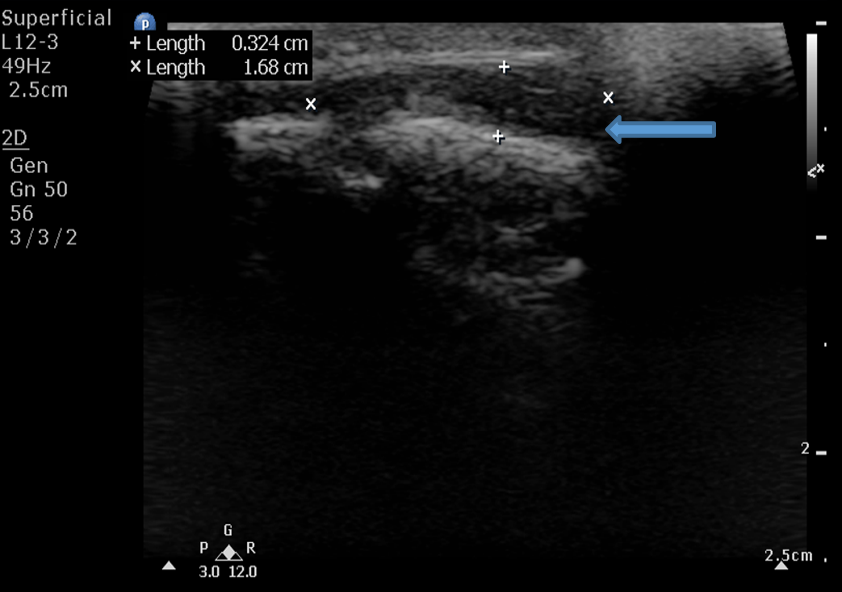
- A. Hypoechoic soft tissue lesion in the subgaleal location measuring 3 x 17mm over frontal region in the midline with a small defect in the underlying calvarium.
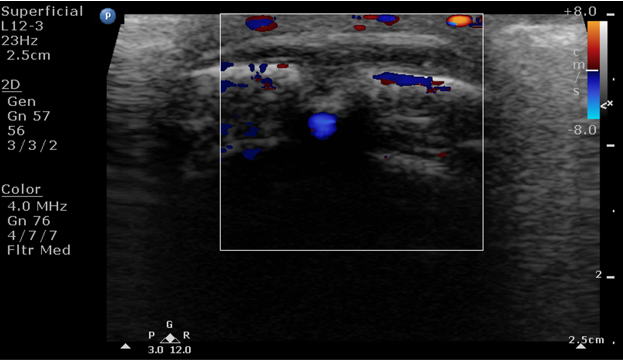
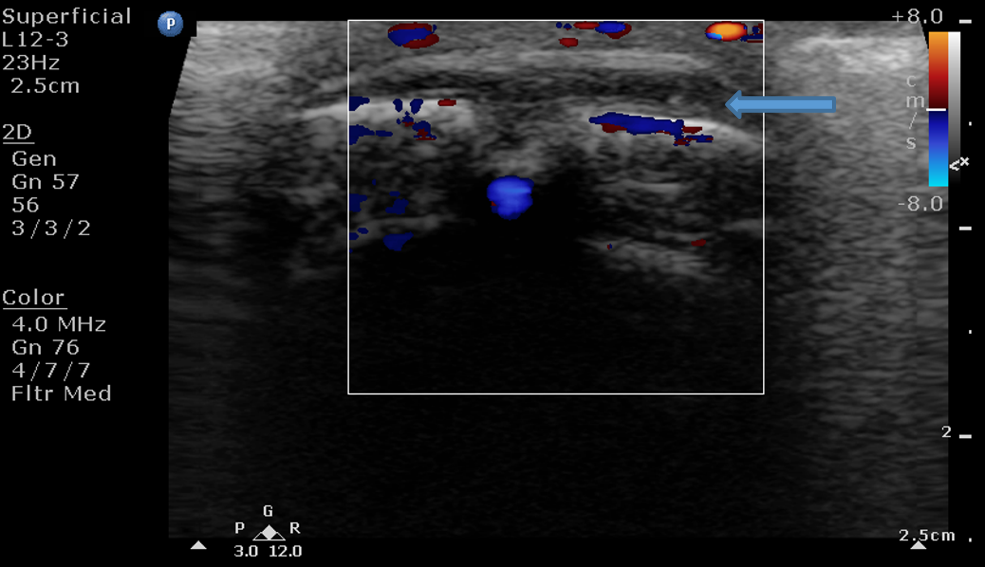
- No vascularity on doppler evaluation. No collection.
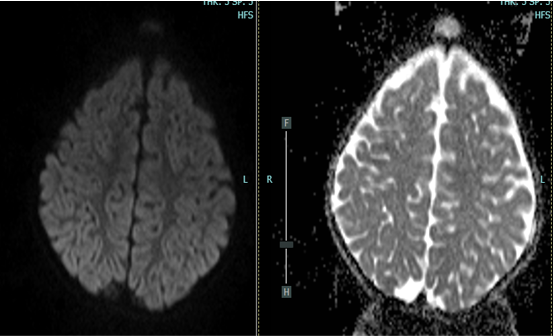
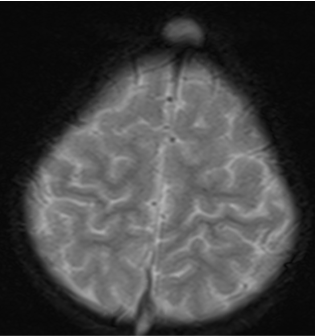
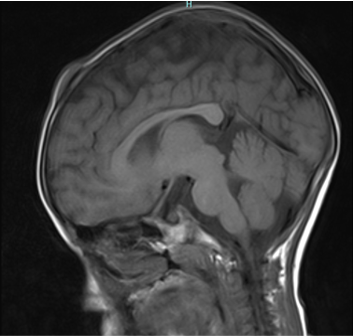
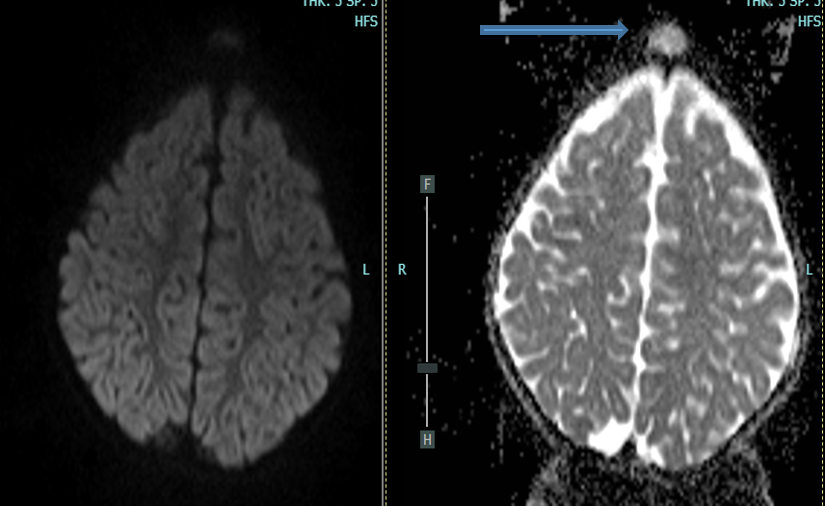
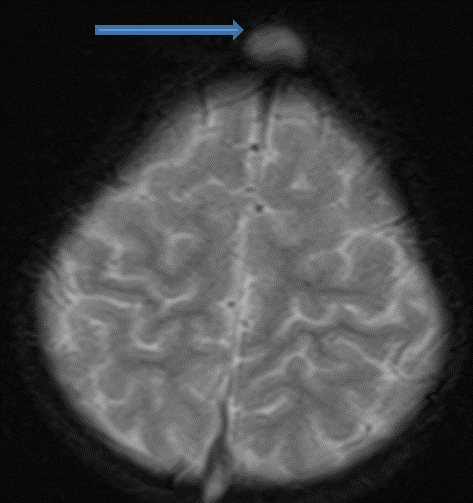
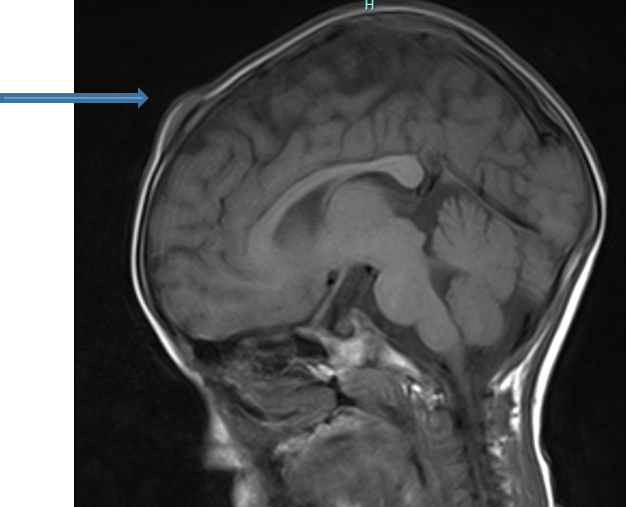
- B. Well-defined, extra-axial T2 hyperintense, T1 isointense, soft tissue lesion with no diffusion restriction in the midline frontal region.
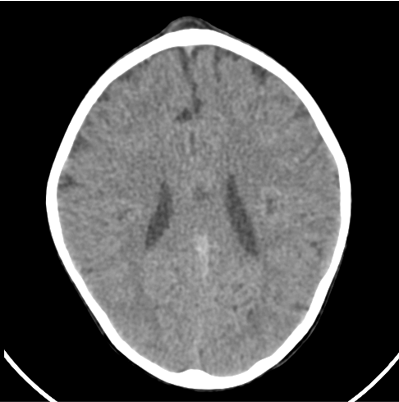
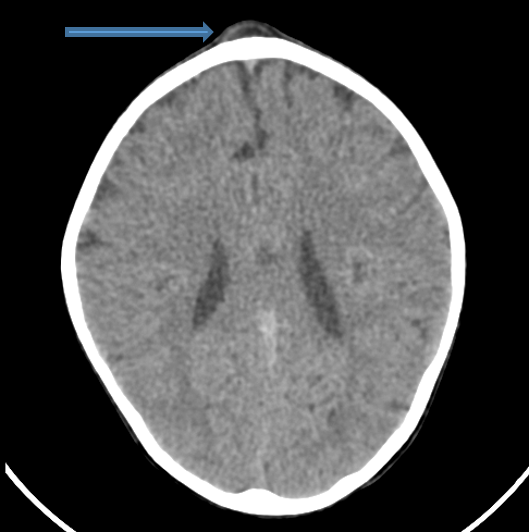
- C.Correlative CT shows a fat density lesion. No intra-lesional calcification.
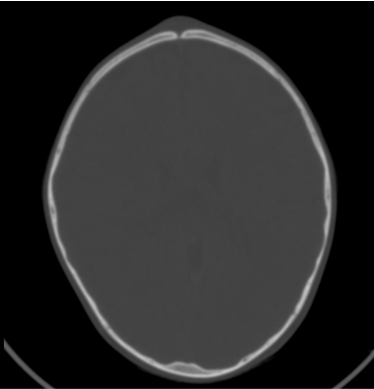
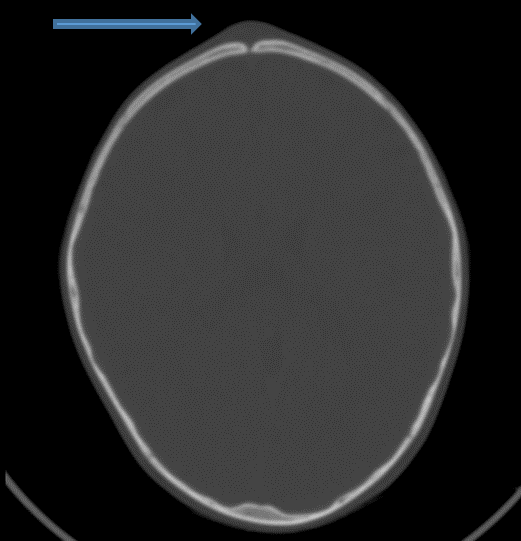
- The underlying frontal bone shows mild scalloping of the outer table with a small defect/ sinus tract of length 3mm reaching up to the dura. No communication with the patent superior sagittal sinus. Underlying brain parenchyma appears normal. No intracranial extension.
DIAGNOSIS
- Midline frontal dermoid cyst with a small sinus tract. No intracranial extension.
DISCUSSION
- A dermoid cyst is a thin-walled benign tumor formed by the entrapment of ectodermal tissue during embryologic development, resulting in the inclusion of epithelium and adnexal elements within the tumor.
- They are not unique to a single anatomic location but are often isolated to the skin and subcutaneous tissue and commonly midline.
- Dermoid cysts are lined by thick squamous epithelium and contain epidermal appendages such as sebaceous glands, sweat glands and hair follicles.
- They usually present in the first 3 decades of life.
- Although rare, it is still , along with Langerhans cell histiocytosis, one of the more common lesions in the pediatric skull.
- On CT, dermoids appear as expansile, osteolytic midline lesions with a soft-tissue component, that can be localized or can extend into the adjacent soft tissues/ intracranially. They have fat attenuation due to sebaceous secretions. Intralesional calcifications can be present.
- On MRI, they have a variable appearance with fat signal intensity on T1-weighted images.
- MRI is vital in the evaluation of these lesions to accurately assess the deeper/ intracranial extent as these can be a conduit to infections and increased morbidity.
- Increased heterogeneity, enhancement and adjacent inflammatory changes should raise a possibility of secondary infection.
DIFFERENTIAL DIAGNOSIS
- Epidermoid
- Langerhans cell histiocytosis
- Encephalocele
- Nasal glioma/ nasal glial heterotopia
- Sinus pericranii.
TREATMENT
- Complete surgical excision, which may require a combined intracranial and extracranial approach.
REFERENCES
- [1] Gomez CK, Schiffman SR, Bhatt AA. Radiological review of skull lesions. Insights Imaging. 2018 Oct;9(5):857-882. doi: 10.1007/s13244-018-0643-0. Epub 2018 Sep 19. PMID: 30232767; PMCID: PMC6206383.
- [2] Wood J, Couture D, David LR. Midline dermoid cyst resulting in frontal bone erosion. J Craniofac Surg. 2012 Jan;23(1):131-4. doi: 10.1097/SCS.0b013e318240fe5e. PMID: 22337389.
- [3] Serrallach BL, Orman G, Hicks MJ, Desai N, Kralik S, Huisman TA. Conventional and advanced MR imaging findings in a cohort of pathology-proven dermoid cysts of the pediatric scalp and skull. The Neuroradiology Journal. 2022;35(4):497-503. doi:10.1177/19714009211059120
Dr RAHUL KARTHIK L
Consultant Radiologist
Manipal Hospital, Yeshwanthpur, Bengaluru.
Dr PRIYANKA ROUT
Radiology resident
Manipal Hospital, Yeshwanthpur, Bengaluru.

