
28 year, female Complaints of long standing pelvic pain since 3yrs. Absent left kidney.
History
- 28 year, female
- Complaints of long-standing pelvic pain since 3yrs.
- Absent left kidney.
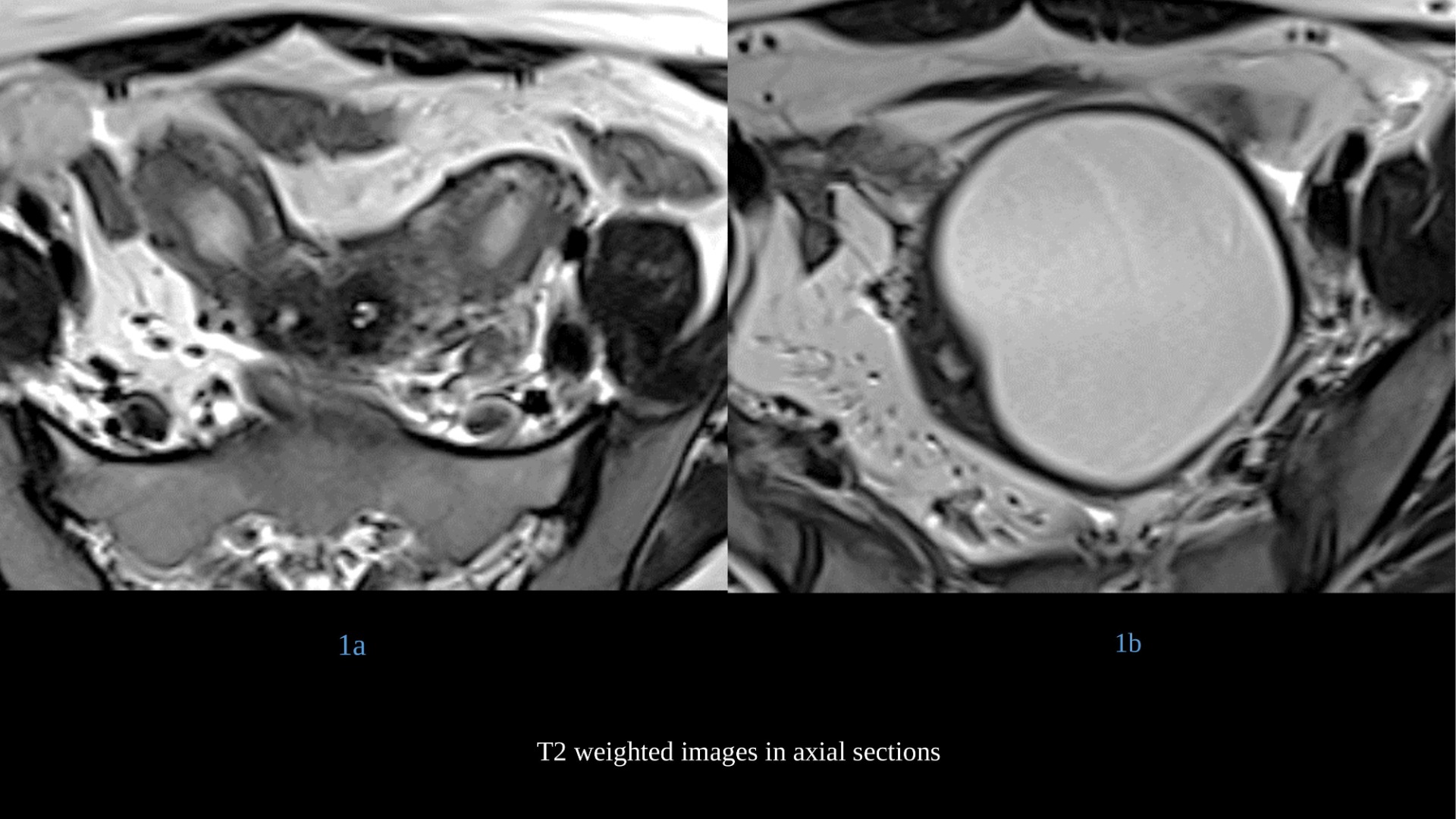
Blue arrow and yellow arrow-
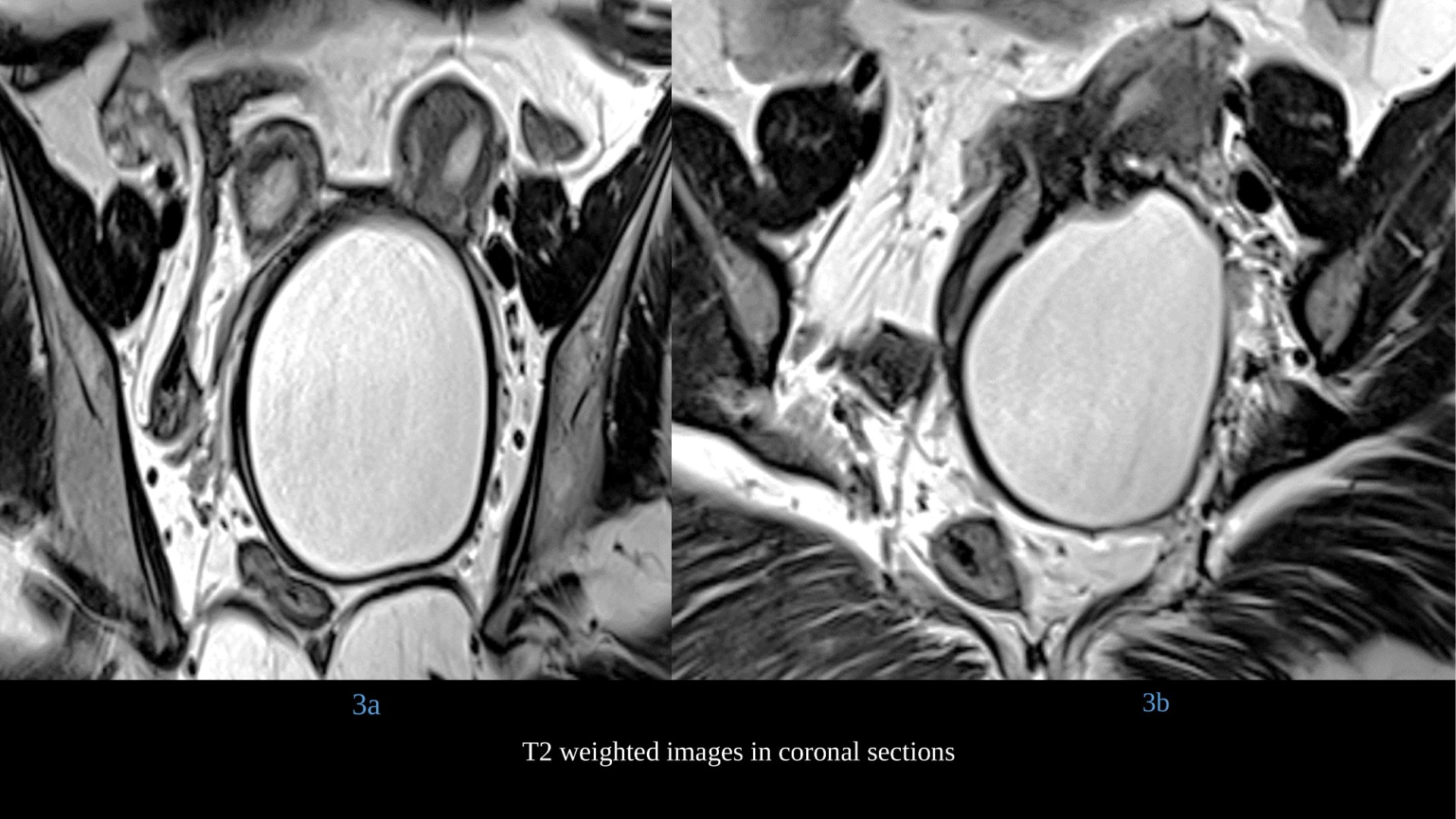
- Two separate uterine bodies with endometrial cavities and cervices.
- Endometrial cavities are unremarkable.
- They communicate with two duplicated vaginal canals.
Red arrow –
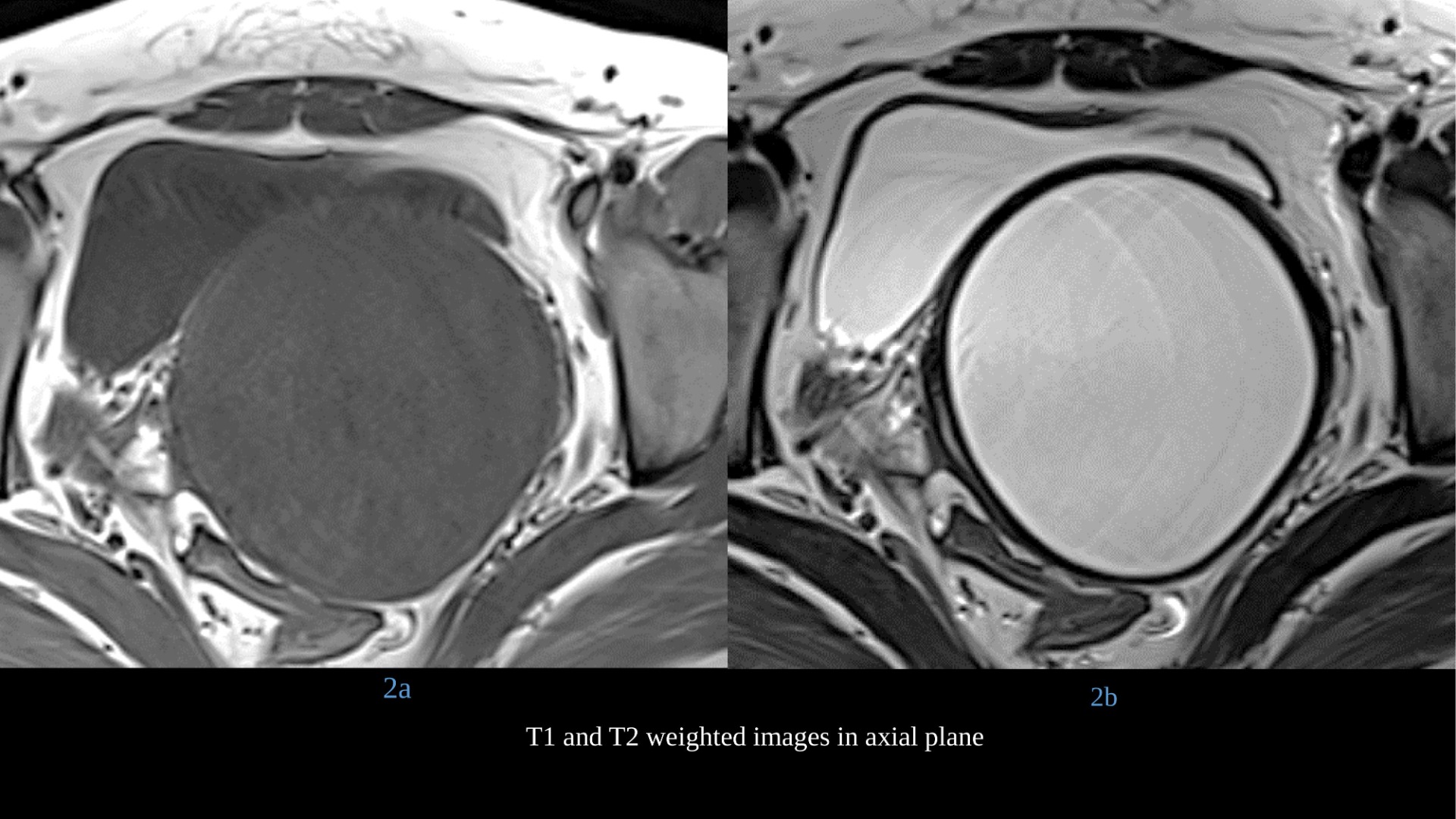
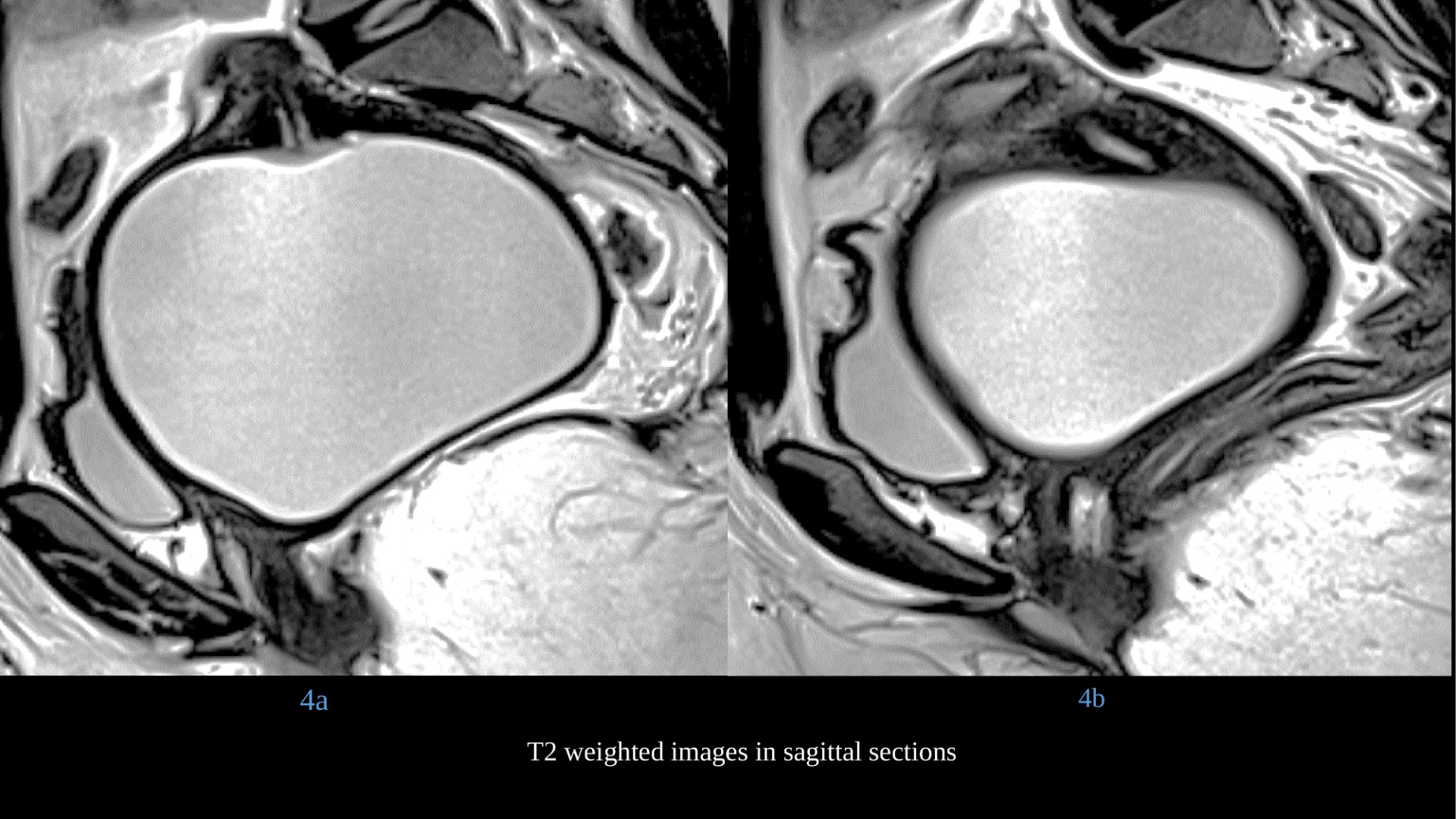
- Left duplicated vaginal canal showing T2 hyperintense and T1 hypointense collection suggestive of hydrocolpos.
Purple arrow –
- No evidence of any collection seen in the right vagina.
Diagnosis : Herlyn-Werner-Wunderlich syndrome / OHVIRA syndrome
DISCUSSION:
- It is a rare complex congenital anomaly of the female genital system.
- It is a triad of obstructed hemi-vagina, uterine didelphys and ipsilateral renal anomaly. Incidence of Mullerian duct anomalies ranges from 0.8% to 4% and the incidence of the OHVIRA syndrome is estimated to be between 0.1-3.5% of all Mullerian anomalies.
- The etiology of the syndrome is unknown. However, it is multifactorial and associated with Mullerian ducts fusion anomalies in utero.
Classical Presentation:
- Young girl presenting with severe dysmenorrhea, few months to years after attaining menarche. Pelvic pain is the most common presenting symptom (90%) followed by an abdominal mass (40%) and pressure symptoms.
- Patients can also present at a later age with foul-smelling vaginal discharge due to pyocolpos.
- Because of regular menstruation in these patients (at menarche), diagnosis is often delayed.
- Patients can present with complications like endometriosis, hydrosalpinx, secondary infection and pelvic adhesions causing chronic pelvic pain.
- If not diagnosed and treated in time, long-term problems like infertility.
Radiology Findings:
- Commonly used are ultrasonography and MRI.
- Ultrasound can diagnose the collection inside the uterus or vagina (secondary to obstruction, and may raise the differential of adenexal masses i.e. endometriomas and cystadenoma), but cannot identify the type of Mullerian anomaly.
- MRI due to its multiplanar and tissue characterization abilities can give precise information about uterine morphology and about the continuity with each vaginal (obstructed and non-obstructed) lumen.
- MRI has more sensitivity in detecting the uterine contour, the shape of the cavity, the presence of a septum, as well as the presence of the associated pathology such as endometriosis, pelvic inflammation, and adhesions.
- Thus MRI is the gold standard method for accurate diagnosis and allows the most appropriate treatment option to be used.
Treatment and outcomes
- Treatment invariably requires surgical intervention in the form of excision of vaginal septum to relieve obstruction.
- Surgery also reduces chances of pelvic endometriosis due to retrograde menstrual seeding.
Differential diagnosis includes:
- Ovarian cystadenoma
- Endometrioma
- Mullerian duct anomaly (Bicornuate uterus)
Summary
- OHVIRA syndrome is an uncommon congenital anomaly with clinical significance and simple surgical management.
- MRI plays a major role in diagnosis, which is often missed clinically.
- Early appropriate surgery helps preventing complications, caused by retrograde menstruation which may result in endometriosis and also preserve sexual and conception abilities.
References
- Resetkova N, Christianson M, Kolp L. (2012) Uterinedidelphys with obstructed hemivagina and ipsilateral renal agenesis with hydronephrosis. Fertil Steril 97:s30-1.
- Dhar H, Yasser AR, Illham H. (2011) Uterusdidelphys with obstructed hemi vagina, ipsilateral renal agenesis and right pyocolpos: a case report. Oman Med J 26:447-50. (PMID: 22253958)
- Saxena N, Channawar S, Khadkikar R, Chauhan AR (2014) OHVIRA Syndrome. JPGO Volume 1 Issue 12
- Bhimarao Patil, Rashmi Mysore Nagaraju (2015) Uterine didelphys with obstructed hemivagina and ipsilateral renal anomaly – OHVIRA syndrome: a rare congenital anomaly. ijrcog (3):889-892
- Altchek A, Paciuc J (2009) Successful pregnancy following surgery in the obstructed uterus in a uterus didelphys with unilateral distal vaginal agenesis and ipsilateral renal agenesis:Case report and literature review. J Pediatr Adolesc Gynecol 22:e159–62. (PMID: 19576808)
Dr. Vaibhav Bhandari
Cross-sectional Fellow
Manipal Hospitals Radiology Group (MHRG)
Manipal Hospital, Bengaluru
Dr. Vishwanath Joshi
Consultant Radiologist.
Manipal Hospital Radiology Group (MHRG)
Manipal Hospital, Bengaluru.

