
26 year female presented with history of abdominal pain and fever for 10 days
A 26-year-old female presented with a history of abdominal pain and fever for 10 days.


FINDINGS
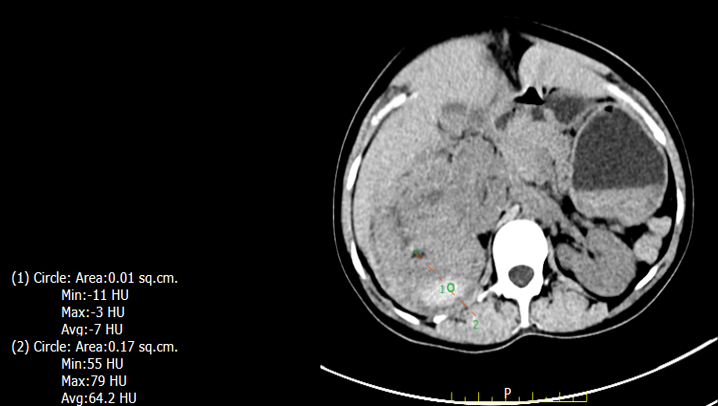
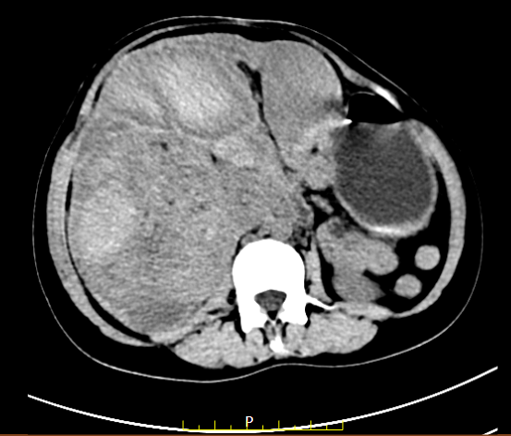
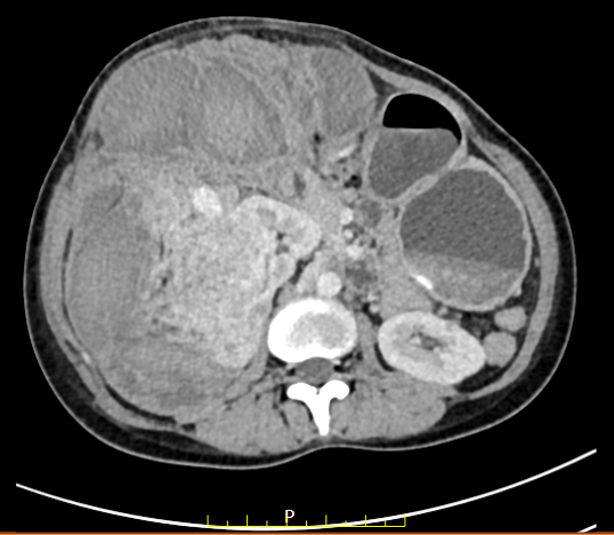
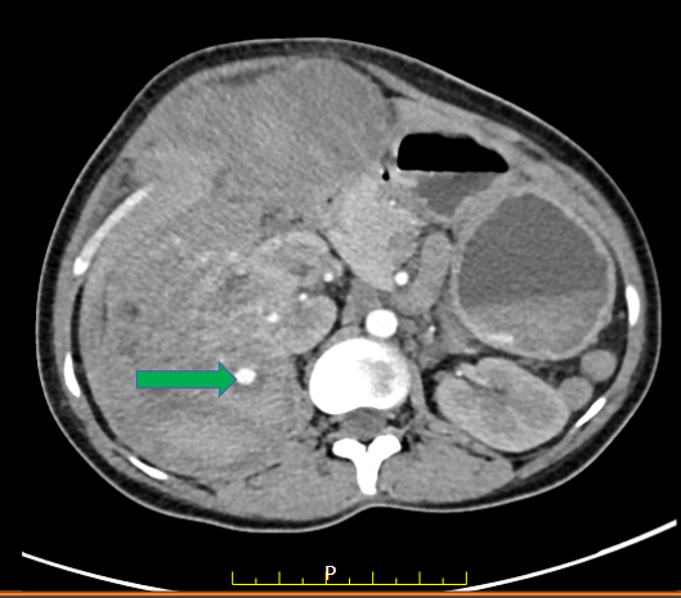
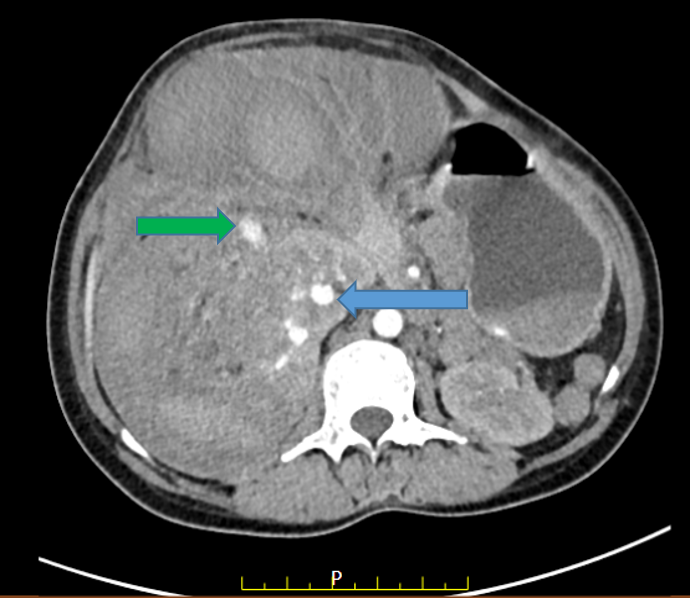
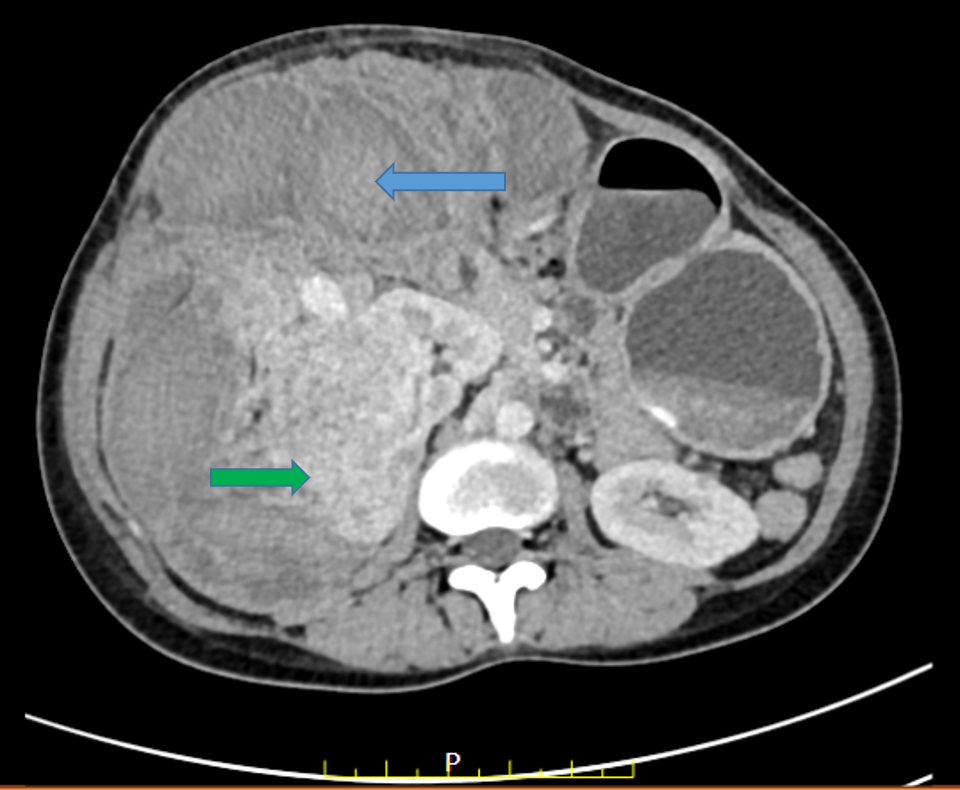
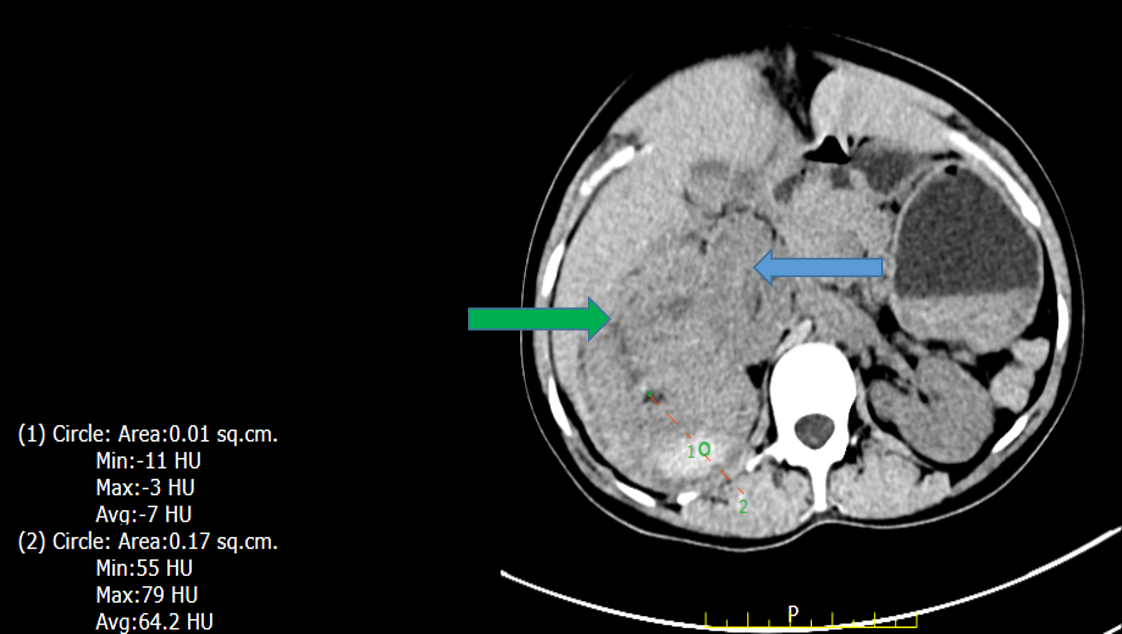
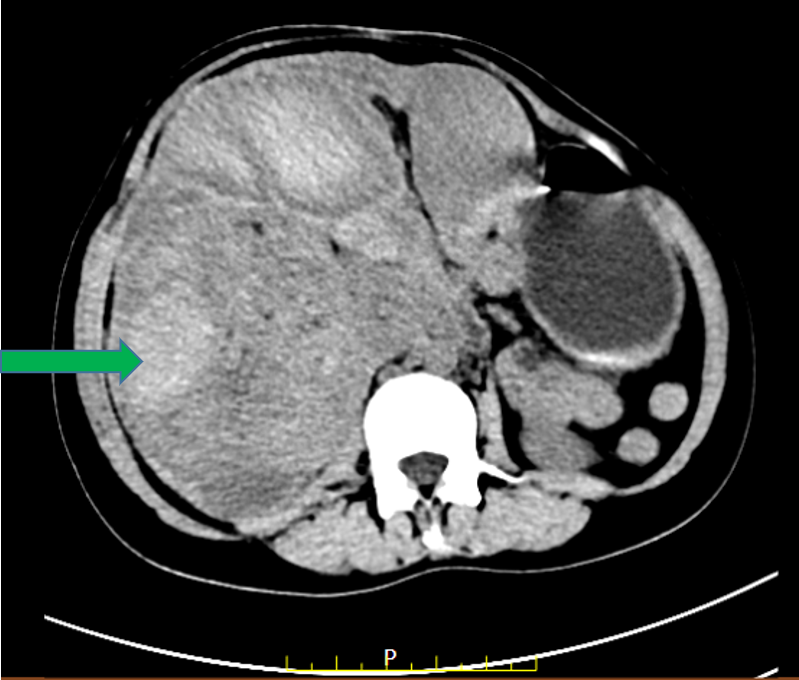
- Large heterogeneously enhancing retroperitoneal lesion seen arising from the mid pole of right kidney with areas of fat and hemorrhage within. Surrounding large perinephric hematoma was seen.
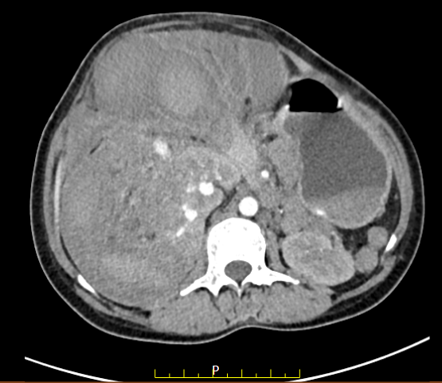
- Few arterial hyper-enhancing foci were seen within the mass lesion and within the right kidney with retention of contrast on the venous phase suggestive of focal aneurysms.
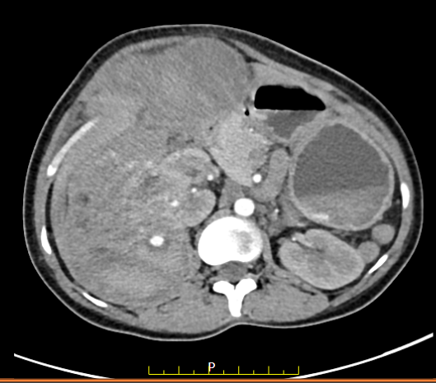
- The lesion is pushing the right kidney anteromedially extending beyond the rota’s fascia into the mesentery and omentum anteriorly.
- The lesion is also pushing the pancreas medially and displacing the adjacent bowel loops.
- Superiorly it is abutting the right lobe of the liver and gallbladder.
- Posteriorly it is abutting the posterior abdominal wall and medially the right psoas muscle.
- The left kidney shows a tiny fat-containing lesion measuring 8 x 7 mm in the lower pole region. No perinephric collection was seen.


DIAGNOSIS:
WUNDERLICH SYNDROME SECONDARY TO RUPTURED RIGHT RENAL ANGIOMYOLIPOMA AND ASSOCIATED MODERATE PERINEPHRIC HEMATOMA AND ANEURYSMS.
WUNDERLICH SYNDROME:
- Wunderlich syndrome (WS) refers to spontaneous renal or perinephric hemorrhage occurring in the absence of known trauma. WS is much less common than hemorrhage occurring after iatrogenic or traumatic conditions.
- Wunderlich syndrome is eponymously named after Carl Wunderlich, who first described a patient with spontaneous subcapsular and perinephric bleeding without preceding trauma in 1856.
- Trauma and iatrogenic causes such as recent biopsy or surgical procedure need to be excluded prior to labeling as WS. More than two-thirds of patients present with flank pain as the presenting symptom.
- A wide spectrum of neoplastic and non-neoplastic renal pathologies may result in WS.
- Renal neoplasms are the most common cause for WS, with angiomyolipoma being the most common benign neoplasm, whereas renal cell carcinoma is the most common malignant neoplasm.
- CT helps in the detection of the subcapsular and/or perinephric hemorrhage and may identify underlying etiology.
- Renal angiography not only helps in diagnosis of the underlying cause in select cases but also allows control of active bleeding, which can avoid unnecessary emergent radical surgery.
- Therapeutic embolization and nephrectomy are the treatment options for Wunderlich’s syndrome.
RENAL ANGIOMYOLIPOMAS:
- Angiomyolipomas (AMLs) are the most frequent benign renal tumour, with a prevalence varying between 0.2% and 0.6% and a strong female predilection.
- They occur as sporadic, isolated entities in 80% of cases.
- The remaining 20% of AMLs develop in association with tuberosclerosis complex (TSC) or pulmonary lymphangioleiomyomatosis (LAM).

DIFFERENTIAL DIAGNOSIS:
- Radiological distinction between non-classic AMLs and RCCs continues to be difficult.
- Clinical information supporting a diagnosis of AML includes a younger age, female sex, and asymptomatic presentation.
- Imaging findings that should raise the suspicion of AML include:1. Absence of calcification,
2. Absence of perinephric collateral vessels,
3. Multiple lesions,
4.Hyperattenuation in comparison to renal parenchyma on plain CT, and hypointensity on T2-weighted MRI. - However, no single finding or modality is perfectly accurate; such cases need biopsy or surgical excision.
REFERENCES
- Parmar N, Langdon J, Kaliannan K, Mathur M, Guo Y, Mahalingam S. Wunderlich syndrome: wonder what it is. Current Problems in Diagnostic Radiology. 2022 Mar 1;51(2):270-81.
- Katabathina VS, Katre R, Prasad SR, Surabhi VR, Shanbhogue AK, Sunnapwar A. Wunderlich syndrome: cross-sectional imaging review. Journal of computer-assisted tomography. 2011 Jul 1;35(4):425-33.dicine. 2017 May 1;130(5):e217-8.
- Vos, N and Oyen, R. Renal Angiomyolipoma: The Good, the Bad, and the Ugly. Journal of the Belgian Society of Radiology. 2018; 102(1): 41, pp. 1–9. DOI: https://doi.org/10.5334/jbsr.1536.
Dr. Nikita Patel
Cross-sectional Fellow
Manipal Hospital Radiology Group (MHRG)
Manipal Hospital, Bengaluru
Dr. Vishwanath Joshi
Consultant Radiologist.
Manipal Hospital Radiology Group (MHRG)
Manipal Hospital, Bengaluru.
