

22-year-old gravid lady with abdominal pain and anuria for one day. Left solitary kidney. S/p left pyeloplasty one year back.
22-year-old gravid lady with abdominal pain and anuria for one day. Left solitary kidney. S/p left pyeloplasty one year back.
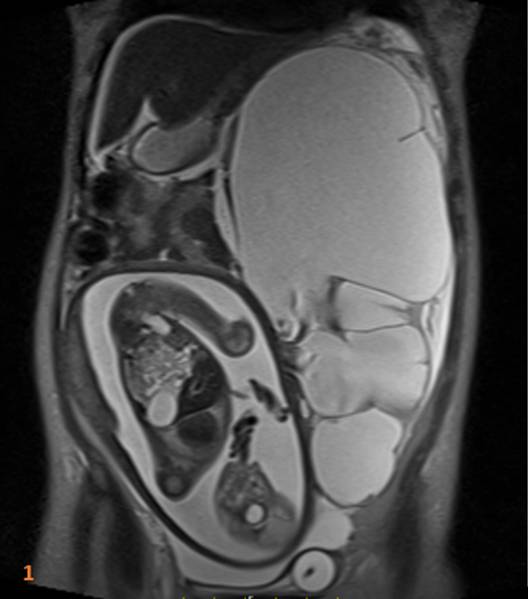

- Severe left hydronephrosis with significant renal parenchymal thinning (Fig.1a) Gravid Uterus with a single intrauterine fetus, normal placenta for age and normal fetal parts.
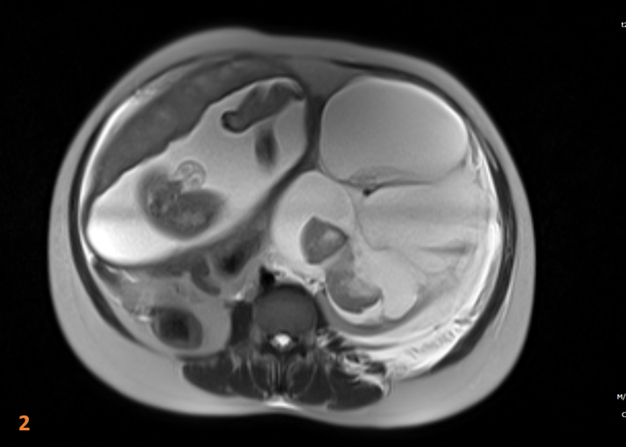
- Left perinephric urinoma with large acute to subacute hematoma and apparent breach of posterior pyelo-parenchymal junction (red arrow in Fig.2a and 3a). Fluid seen in the left posterior peri-renal space tracking along the left para-spinal muscles and posterior abdominal wall (green arrows in Fig.3a).
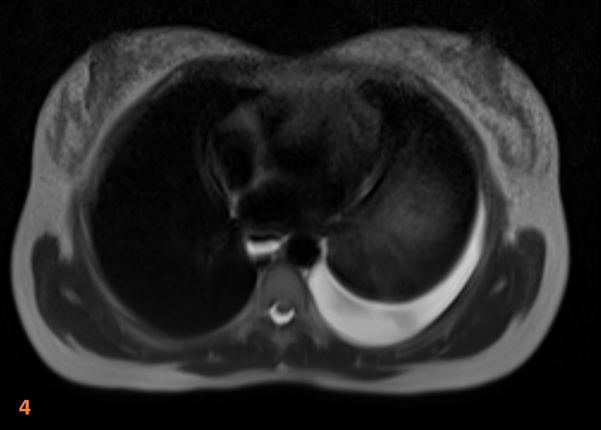
- Mild ascites with mild to moderate left pleural effusion (Fig.4a)
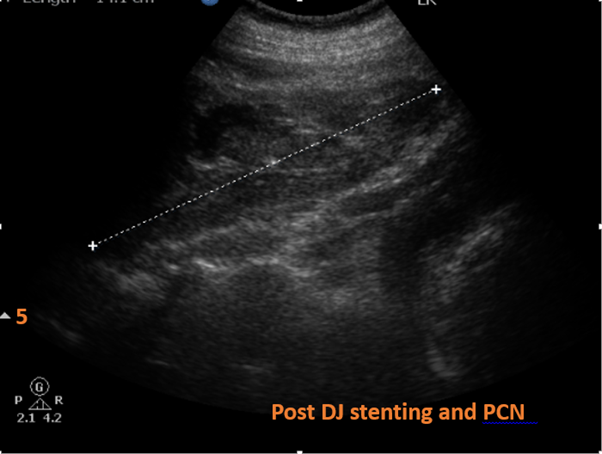
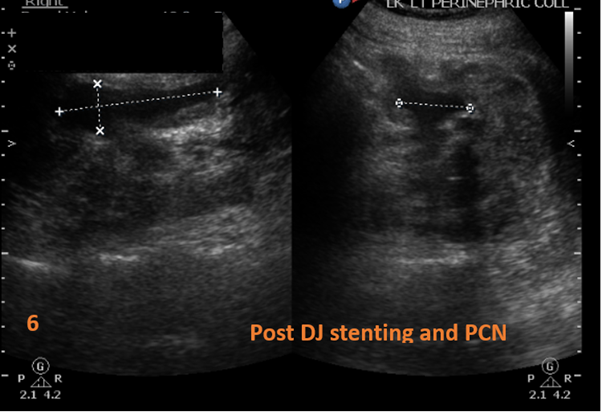
- Interval resolution of hydronephrosis and significant reduction of perinephric urinoma post DJ stenting and PCN (Fig.5a and 6a).
Diagnosis:
Spontaneous perinephric urinoma with intrarenal hematoma in pregnancy.
Discussion:
- Urinoma is a continued perinephric or peripelvic extravasation of urine leading to the formation of an encapsulated retroperitoneal urine collection.
- Trauma or surgery to the ureter, infection and nephrolithiasis are known causes of non-obstetric urinoma.
- Spontaneous maternal urinoma is a rare complication of hydronephrosis even in a normal kidney during pregnancy.
- Maternal urinoma is thought to develop secondary to the rupture of the calyceal fornix. It occurs when renal pelvis pressure exceeds a critical level between 70 and 75 mmHg due to ureteral or renal compression and often presents with hematuria.
- Ureteral stent placement is an essential treatment for maternal urinoma as ureteral compression by gravid uterus is the underlying pathophysiology.
- This case was unique in that the patient had a solitary left kidney with congenital PUJ with a functioning pyeloplasty prior to pregnancy, but developed a spontaneous urinoma with anuria and rising Serum creatinine at 25 weeks.
- The patient underwent rapid percutaneous nephrostomy and ureteral stenting resulting in rapid decline in elevated creatinine and a decompressed left kidney as seen in follow up Ultrasound images.
REFERENCES/ FURTHER READING:
- Chen, Y., Yan, Y.F., Zhang, Y. et al.Perinephric urinoma following spontaneous renal rupture in the third trimester of pregnancy: a case report and brief review of the literature. BMC Pregnancy Childbirth 19, 505 (2019).
- Ushioda, N., Matsuo, K., Nagamatsu, M., Kimura, T., & Shimoya, K. (2008). Maternal urinoma during pregnancy. Journal of Obstetrics and Gynaecology Research, 34(1), 88–91.
- Hamoud, K., Kaneti, J., Smailowitz, Z. et al. Spontaneous perinephric urinoma in pregnancy. International Urology and Nephrology 26, 643–646 (1994).
- Mandal D, Saha MM, Pal DK. Urological disorders and pregnancy: An overall experience. Urol Ann. 2017;9(1):32-36.
Dr. Sunita Gopalan
DMRD, FRCR
Senior Consultant Radiologist
Manipal Hospitals Radiology Group.
Dr. Suvarna Kote
Radiology resident- Manipal Hospitals Radiology Group.

