
A 69-year-old with history of left parotidectomy for mucoepidermoid carcinoma of parotid gland. On follow up.
A 69-year-old with a history of left parotidectomy for mucoepidermoid carcinoma of the parotid gland. On follow-up.

A. Post left side parotidectomy. Right parotid gland is normal(orange arrow). Ill-defined heterogeneously enhancing mass(blue arrow) with central areas of necrosis in the left parotid surgical bed.
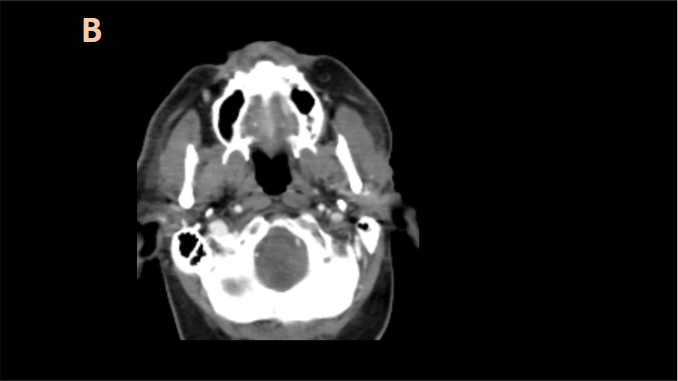
B. Medially, there is extension of the enhancing soft tissue beyond the retro-mandibular margin along the normal course of auriculo-temporal nerve(white arrow) abutting the postero-lateral margin of lateral pterygoid with fat stranding seen in the parapharyngeal space comparing to contralateral side (orange arrow).
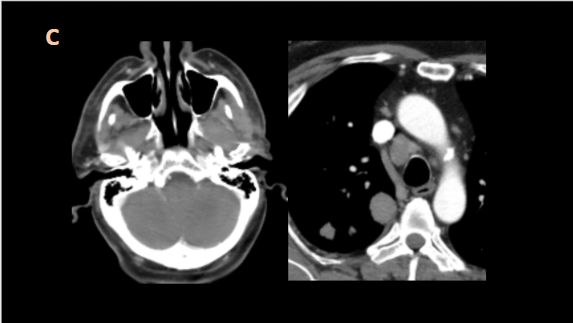
C. Laterally, there is soft tissue thickening seen in the anterior wall of external auditory canal and ear lobule (blue arrow). Multiple randomly distributed soft tissue nodules in both the lungs(orange arrow) and enlarged lymph nodes in mediastinum (white arrow).
DIAGNOSIS:
Local recurrence of mucoepidermoid carcinoma of the left parotid gland with perineural spread along auriculotemporal nerve along with mediastinal nodal and lung parenchymal metastases.
DISCUSSION:
PERINEURAL SPREAD ALONG AURICULOTEMPORAL NERVE
- Perineural invasion occur in SCC, adenoid cystic carcinoma (highest association), mucoepidermoid tumour, melanoma (desmoplastic type), lymphoma.
- Knowledge of the position and course of the auriculotemporal nerve is crucial in diagnosing perineural tumor spread along this branch in patients with known skin lesions or parotid gland tumors.
- The auriculotemporal nerve is one of the major known communications between the facial and trigeminal nerves.
- It arises as two nerve roots from V3 that course posteroinferiorly around the middle meningeal artery—the upper and lower roots extend lateral and medial to the artery, respectively—and coalesce into a short trunk medial to the TMJ and superior to the bifurcation of the external carotid artery into its temporal and maxillary branches. From there, it divides into multiple branches, including the anterior and posterior communicating rami that join the facial nerve within the parotid gland to supply sensory fibres to its zygomatic, buccal, and mandibular divisions.
- Although not present in our patient, symptoms suggestive of auriculotemporal nerve involvement include periauricular pain and TMJ dysfunction and/or tenderness.
IMAGING
- Extension of tumour along the usual pathway of auriculotemporal nerve in the plane between the lateral pterygoid muscle & the posterior fasciculi of the tensor veli palatini muscle.
- Direct findings include a large and/or enhancing nerve, and
- Indirect findings include foraminal widening or destruction, loss of adjacent fat planes, and signs of denervation.
References:
1.Perineural Spread in Head and Neck Malignancies: Clinical Significance and Evaluation with 18F-FDG PET/CT Fabio M. Paes, Adam D. Singer, Adam N. Checkver, Ricardo A. Palmquist, Gabriela De La Vega, and Charif Sidani RadioGraphics 2013 33:6, 1717-1736
2. Schmalfuss, I. M. (2002). Perineural Tumor Spread Along the Auriculotemporal Nerve. AJNR
3. Dankbaar, J.W., Pameijer, F.A., Hendrikse, J. et al. Easily detected signs of perineural tumour spread in head and neck cancer. Insights Imaging 9, 1089–1095 (2018). https://doi.org/10.1007/s13244-018-0672-8
4. Chan M, Dmytriw AA, Bartlett E, Yu E (2013) Imaging of Auriculotemporal Nerve Perineural Spread. OMICS J Radiology 2:135. doi: 10.4172/2167-7964.1000135
Dr Naveen SS
DNB resident
Manipal Hospital, Yeshwanthpur