
A 30-year-old lady, with complaints of difficulty in hearing in right ear.
History
A 30-year-old lady, with complaints of difficulty in hearing in the right ear.
Past surgical history of left canal wall down mastoidectomy for chronic to-mastoiditis.
Otoscopy is suggestive of deep retraction of the right tympanic membrane.
Investigation: HIGH RESOLUTION CT- TEMPORAL BONES.
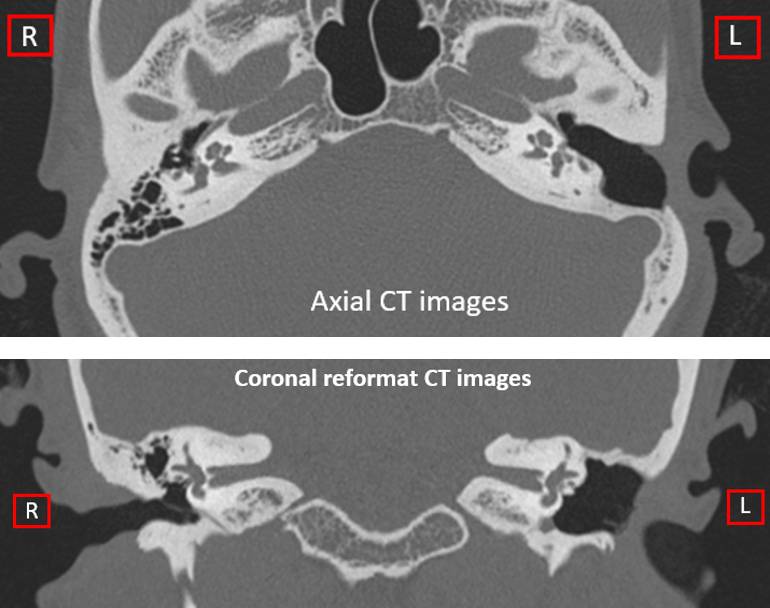
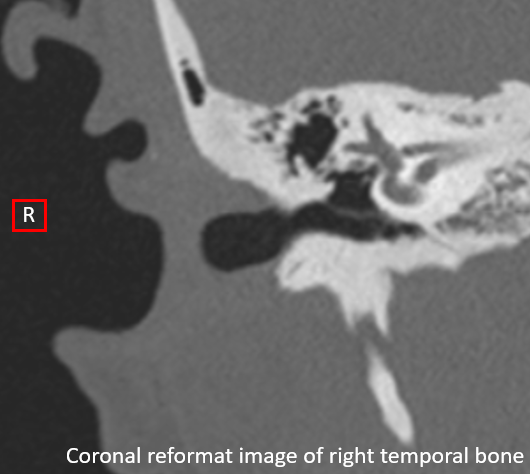
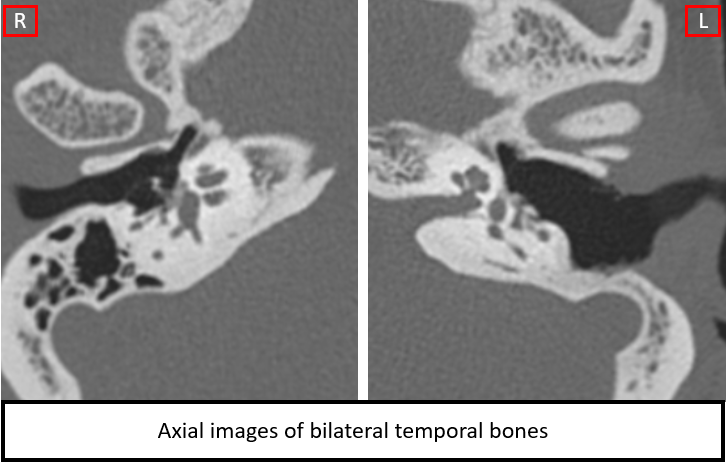
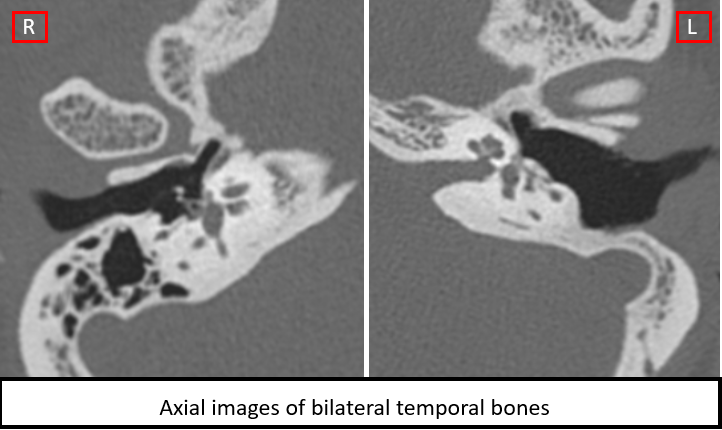
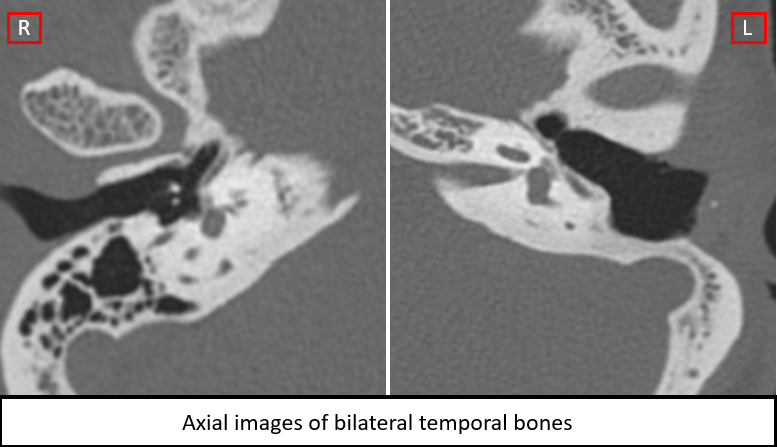
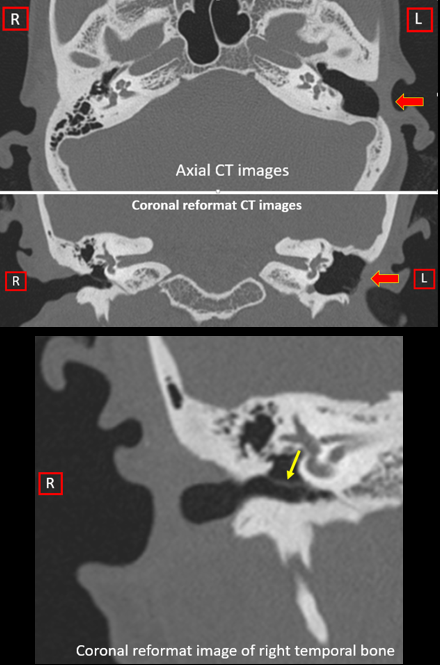
IMAGE 1: CT demonstrates mastoidectomy changes in the left ear (red arrow) and thickened, retracted tympanic membrane (yellow arrow) in the right ear.
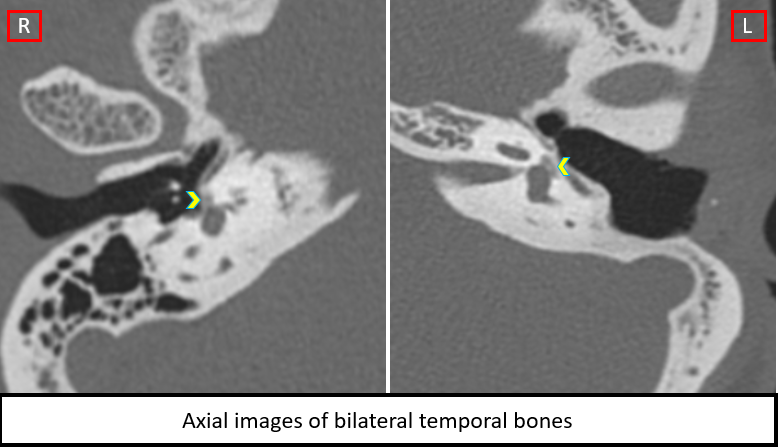
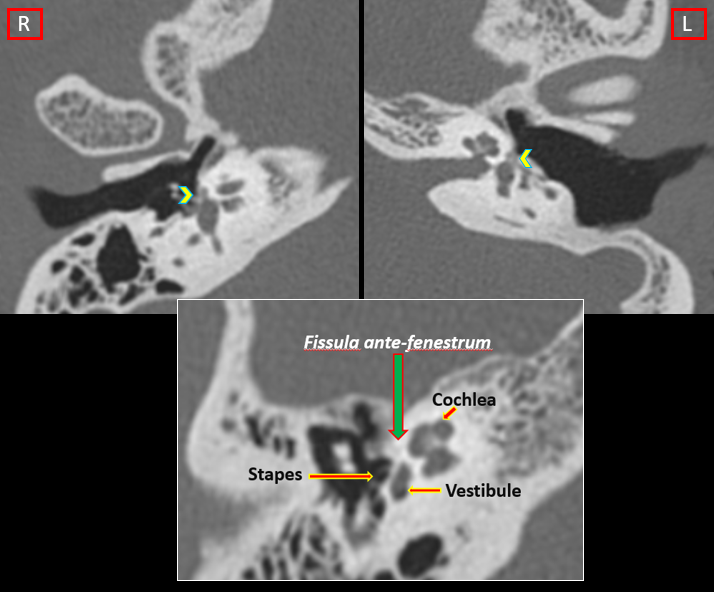
IMAGE 2 & 3: Axial HRCT images demonstrate the focus of demineralization (arrowheads) in the region of the fistula ante fenestrae in bilateral temporal bones.
In image 2 – the normal reference image demonstrates normal dense bone in the region of fistula antefenestrum (seen anterior to vestibule).
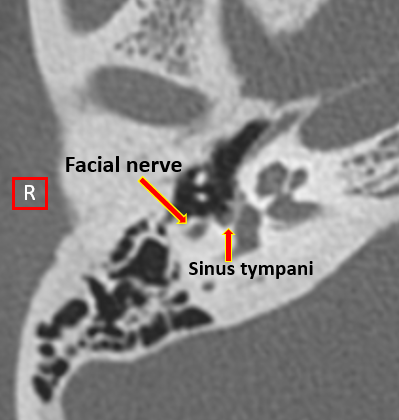
IMAGE 4: Small soft tissue plaque seen in sinus tympani of the right temporal bone, suggestive of heaped-up plaque in continuity with plaque-like demineralization focus in fistula ante fenestra.
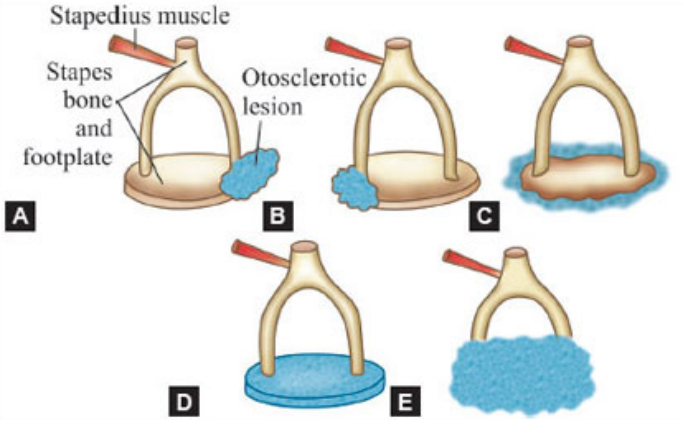
IMAGE 5: Graphic representation of otosclerosis involvement.
- At fissula ante fenestrum.
- At fossula post-fenestram (rare).
- Annular ligament.
- Oval window and footplate of stapes involvement.
- Obliterative otosclerosis – involvement of oval window, footplate and crus of stapes.
DIAGNOSIS AND DISCUSSION:
Diagnosis: Bilateral otosclerosis – Fenestral type.
Discussion:
- In this case, as there was past medical history of oto-mastoiditis in left temporal bone and underwent mastoidectomy and currently, the patient had thickened and retracted tympanic membrane with hearing impairment. The patient was referred to radiology for evaluation of right sided otomastoiditis or cholesteatoma.
- However, on the CT evaluation, the presence of bilateral otosclerosis was identified on imaging.
- Otosclerosis is a disease of otic capsule. It causes conductive or sensory neural or mixed hearing loss.
- Sporadic and autosomal dominant inheritance pattern has been observed.
- Most often occurs in women, in third to fourth decade of life, may be exacerbated by pregnancy.
- It is commonly bilateral and often quite symmetrical.
- Non-contrast high resolution temporal bone CT is considered the gold standard for otosclerosis imaging.
Two types of disease pattern:
- Fenestral type.
- Retro-fenestral type.
Fenestral otosclerosis:
- Involves the lateral wall of the labyrinth, including the promontory, facial nerve canal, and both the oval window and round window niche.
- Oval window involvement is classic as conductive hearing becomes impaired due to stapes fixation.
- In audiometry – Carhart’s notch in bone conduction at 2000 Hz seen in patients with otosclerosis.
In pre-operative CT Evaluation of Otosclerosis, the points that need to be assessed:
- Status of oval window/location of plaques.
- Facial nerve canal (tympanic segment) – for dehiscence/protrusion.
- Jugular bulb – for high riding jugular bulb.
- Round window & Status of cochlea – membranous labyrinthine ossification limited to the basilar cochlear turn and round window involvement have significant implications if cochlear implantation is contemplated.
- Existence of concurrent middle ear disease or congenital ossicular deformity – to rule out other causes hearing impairment.
- Opposite ear – to look for otosclerotic focus.
Treatment:
- The treatment of fenestral otosclerosis is primarily surgical.
Stapedectomy is commonly performed, followed by insertion of a prosthesis.
References:
- Purohit B, Hermans R, Op de Beeck K. Imaging in otosclerosis: A pictorial review. Insights Imaging. 2014;5(2):245-252. doi:10.1007/s13244-014-0313-9
- Mori N, Toyama Y, Kimura N, et al. Detection of small fenestral otosclerotic lesions by high-resolution computed tomography using multiplanar reconstruction. Auris Nasus Larynx. 2013; 40: 36-40.
- Manning, P.M., Shroads, M.R., Bykowski, J. et al. Role of Radiologic Imaging in Otosclerosis. Curr Otorhinolaryngol Rep 10, 1–7 (2022). https://doi.org/10.1007/s40136-021-00377-z
Dr. Diwakar C
Radiology Resident
Manipal Hospital, Yeshwanthopur.