
50 year old female, Post operative history of open cholecystectomy 10 days back.

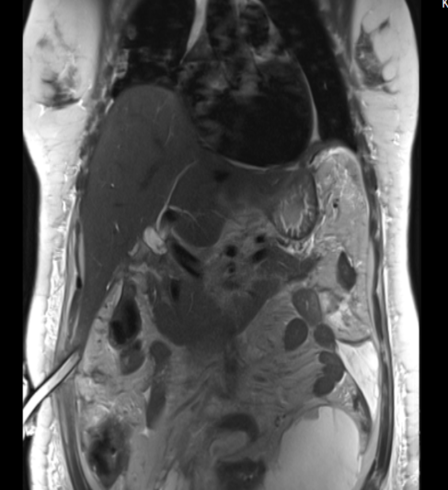
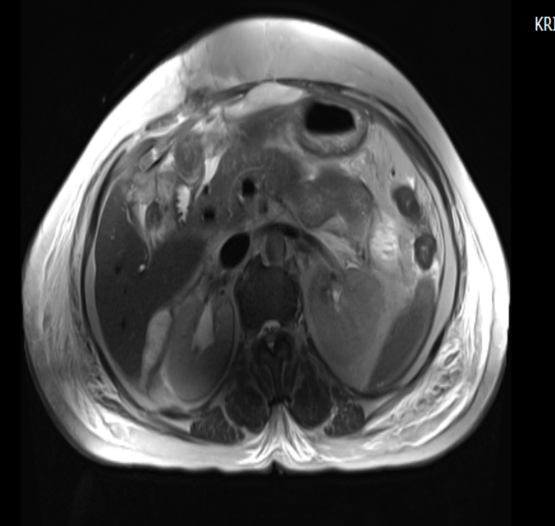
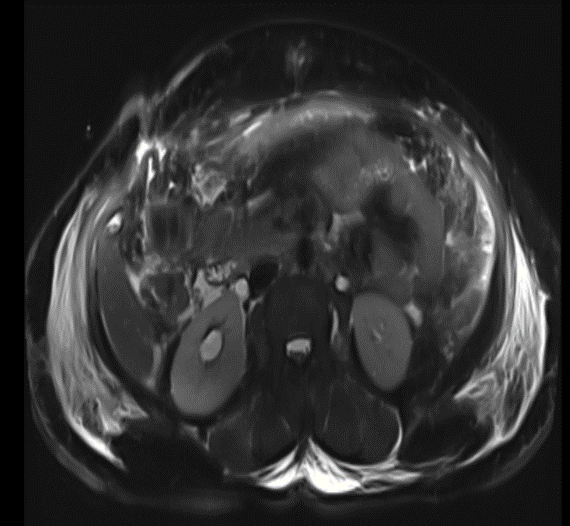
-Gall Bladder not seen – Post cholecystectomy status.
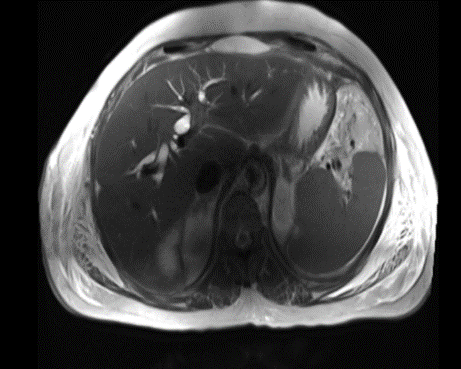
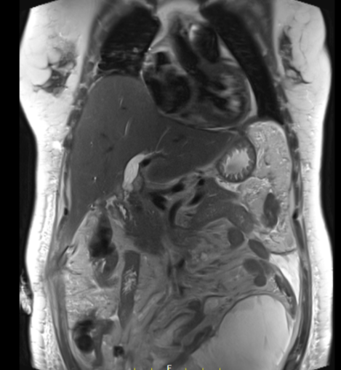
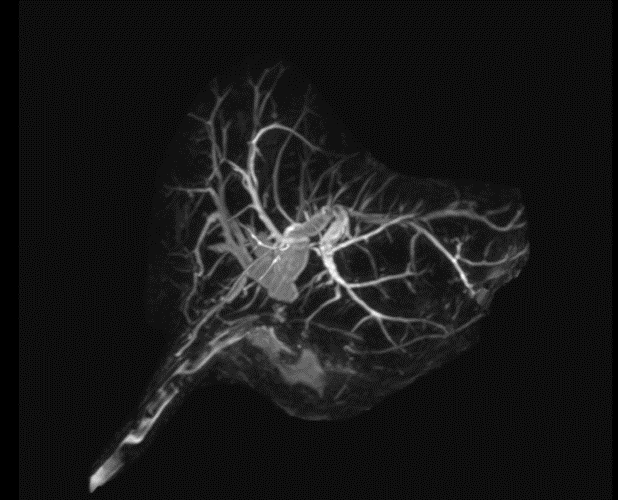
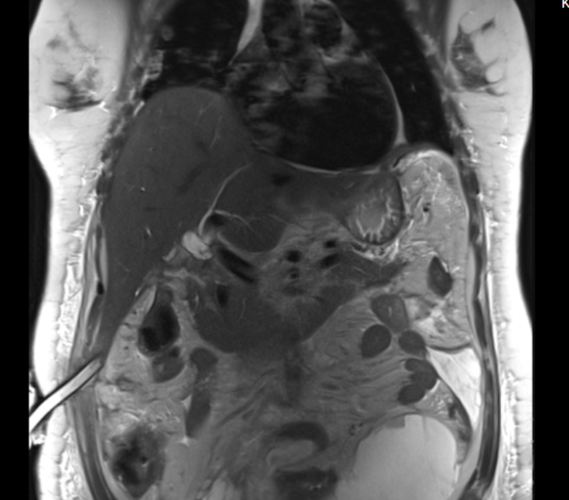
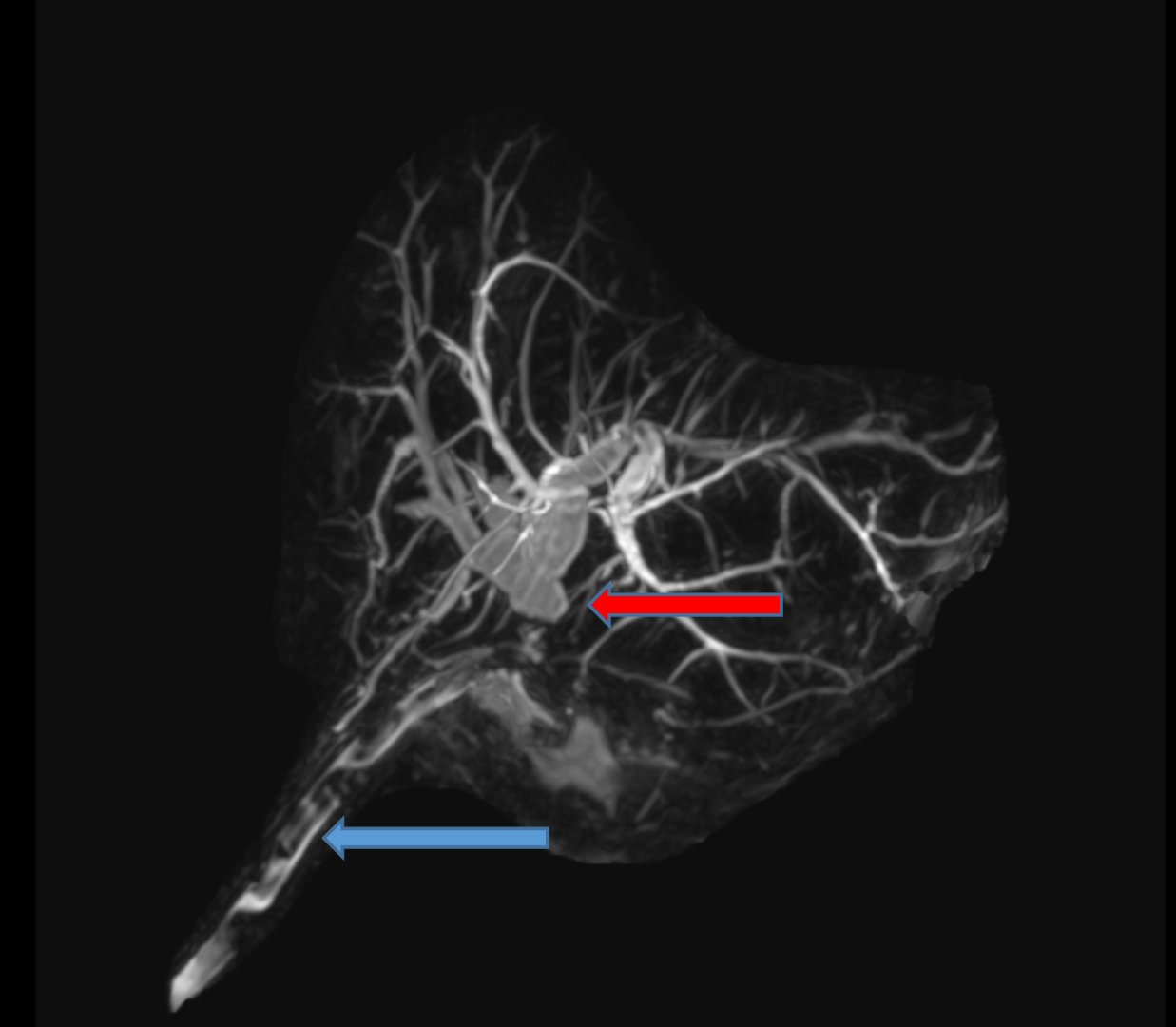
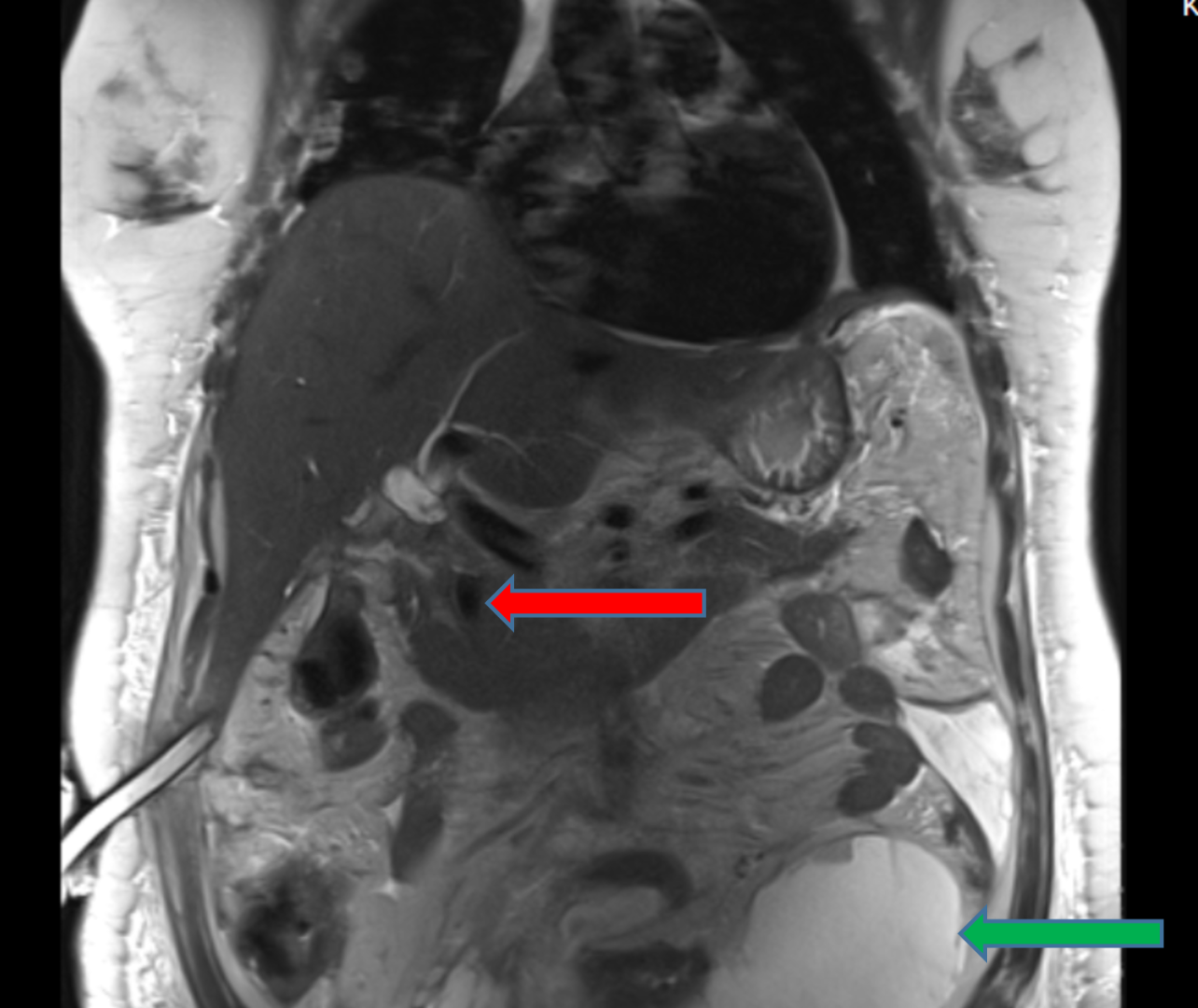
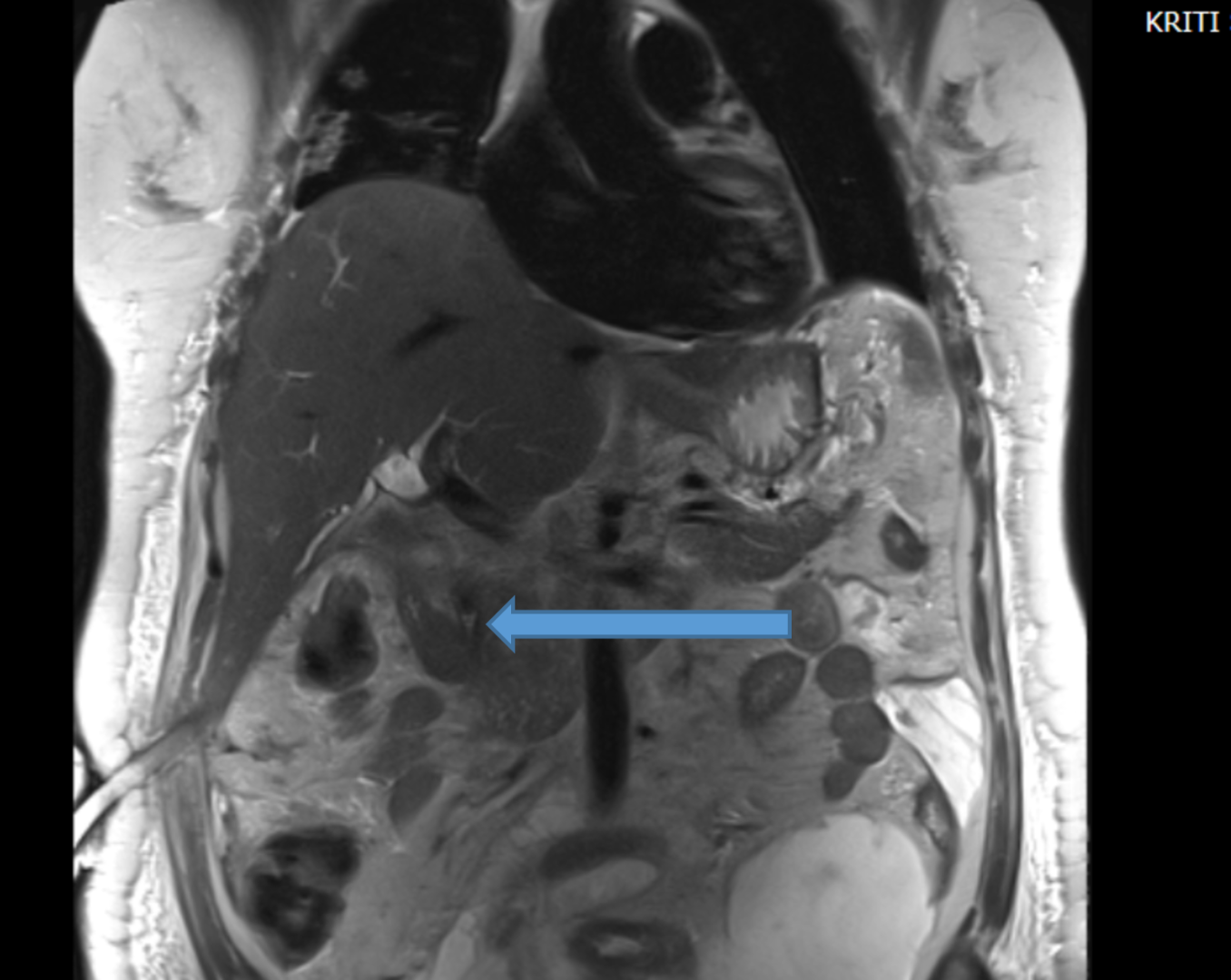
-Dilated bilobar intra hepatic biliary radicals with dilated right and left hepatic duct and confluence with abrupt cut off at the level of proximal common hepatic duct.
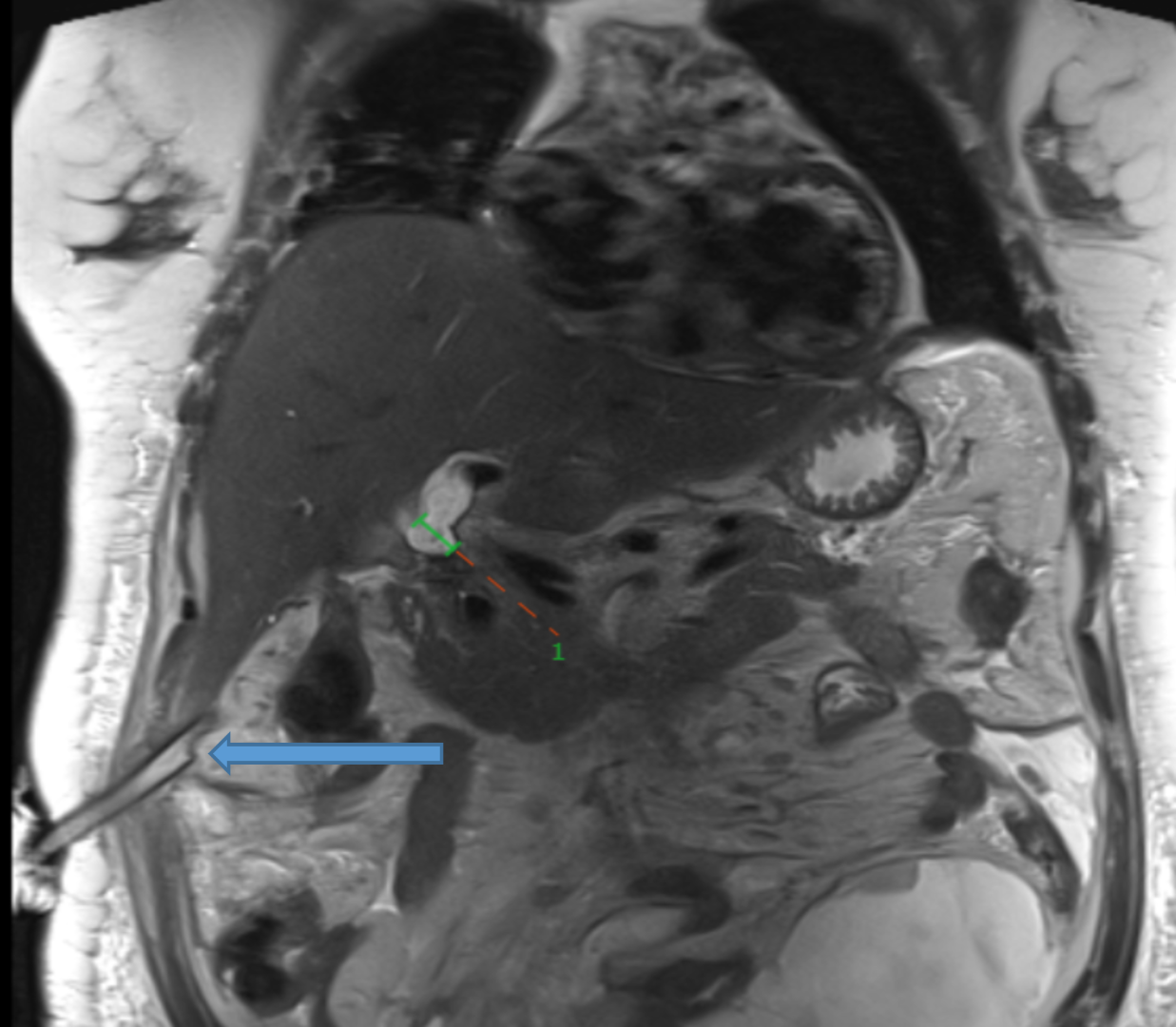
– Distance between confluence and cutoff of proximal common hepatic duct is less then 2 cm.
-15 x 7 mm remnant calculus in the mid-portion common bile duct.
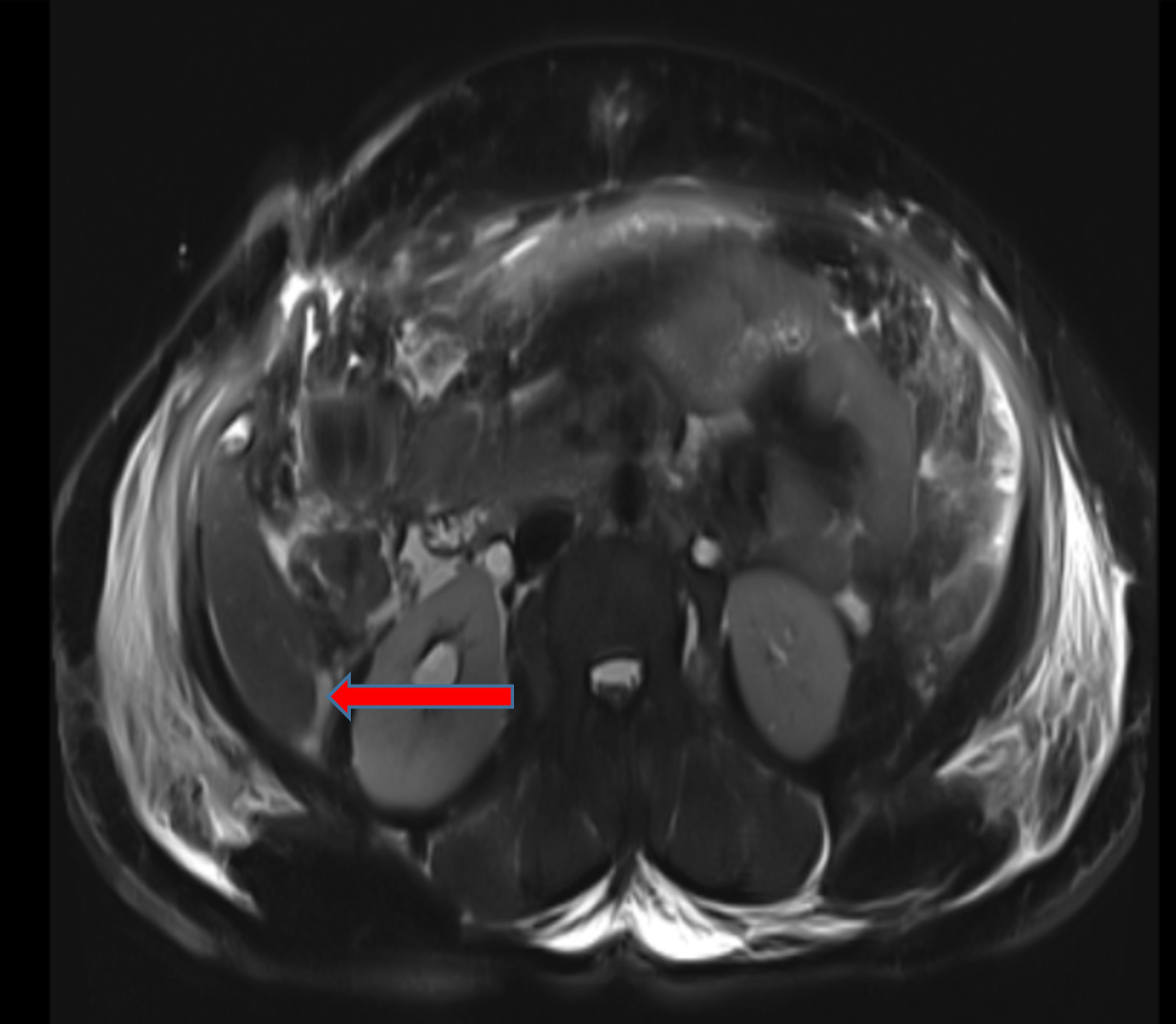
-Post-operative drainage tube in right hypochondriac region with tip in gall bladder fossa.
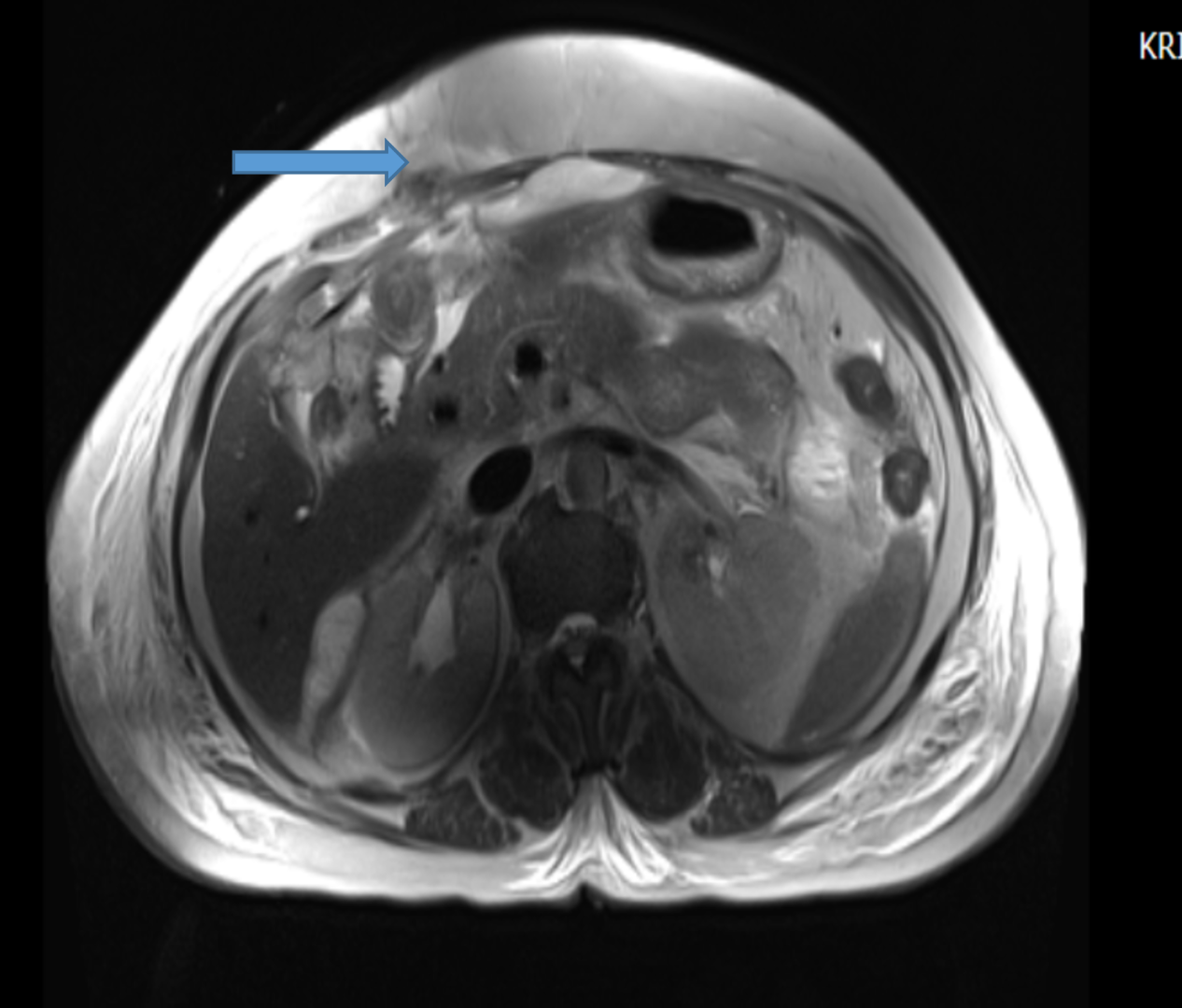
-Mild ascites with diffuse omento-mesenteric fat stranding.
-Loculated fluid collection with internal septations in the abdominal cavity on the left side- likely infected collections/ bilioma.
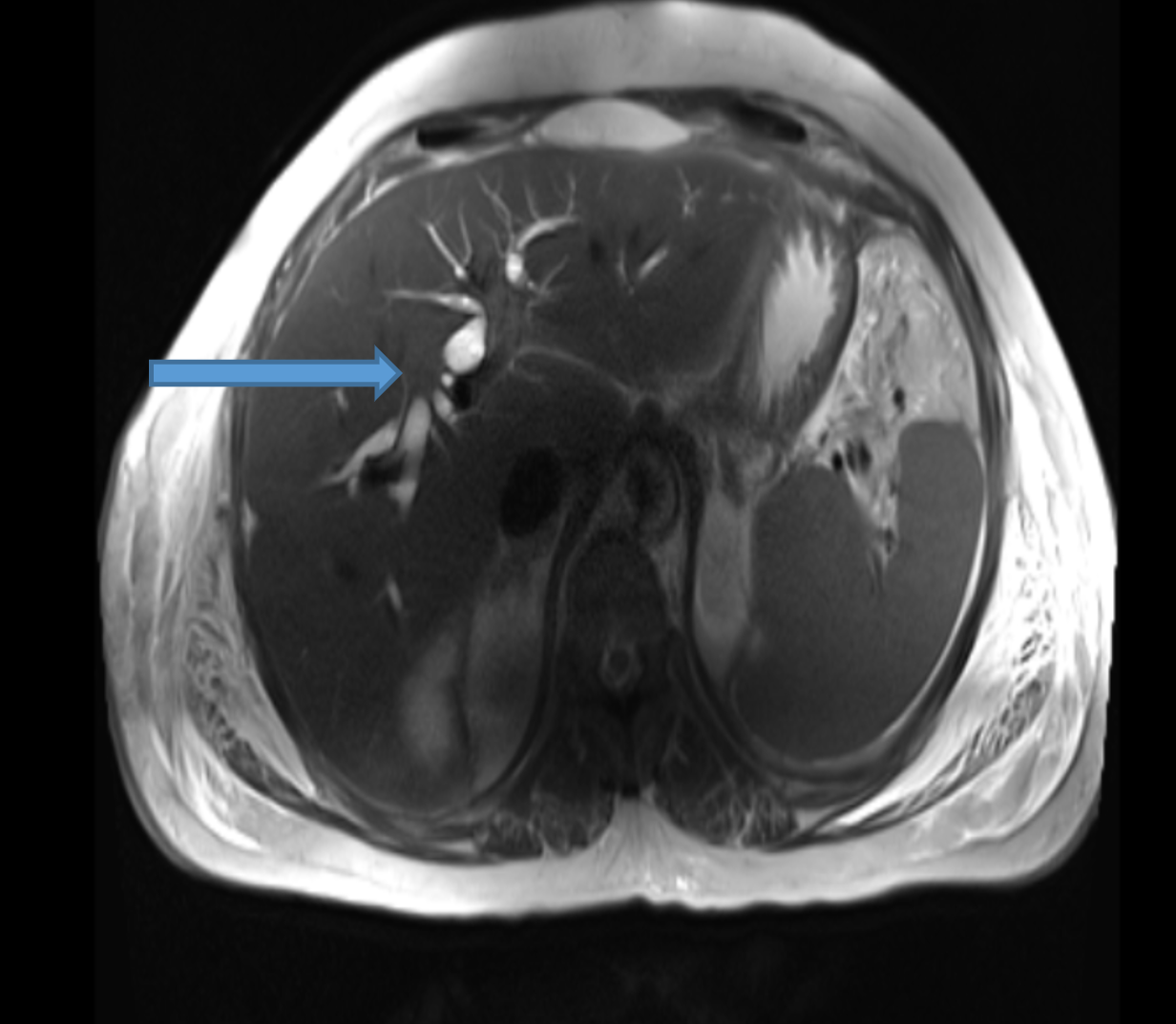
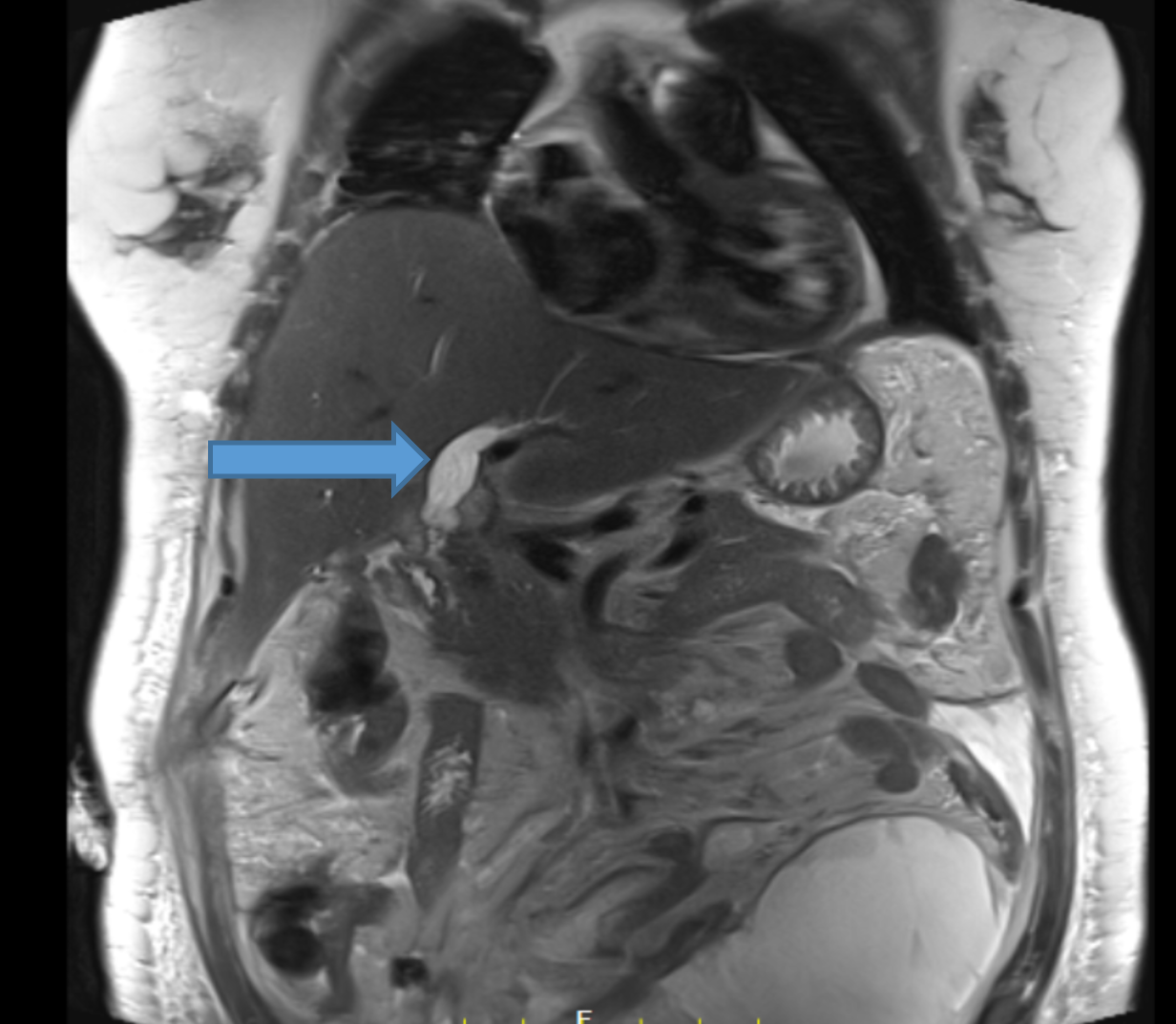
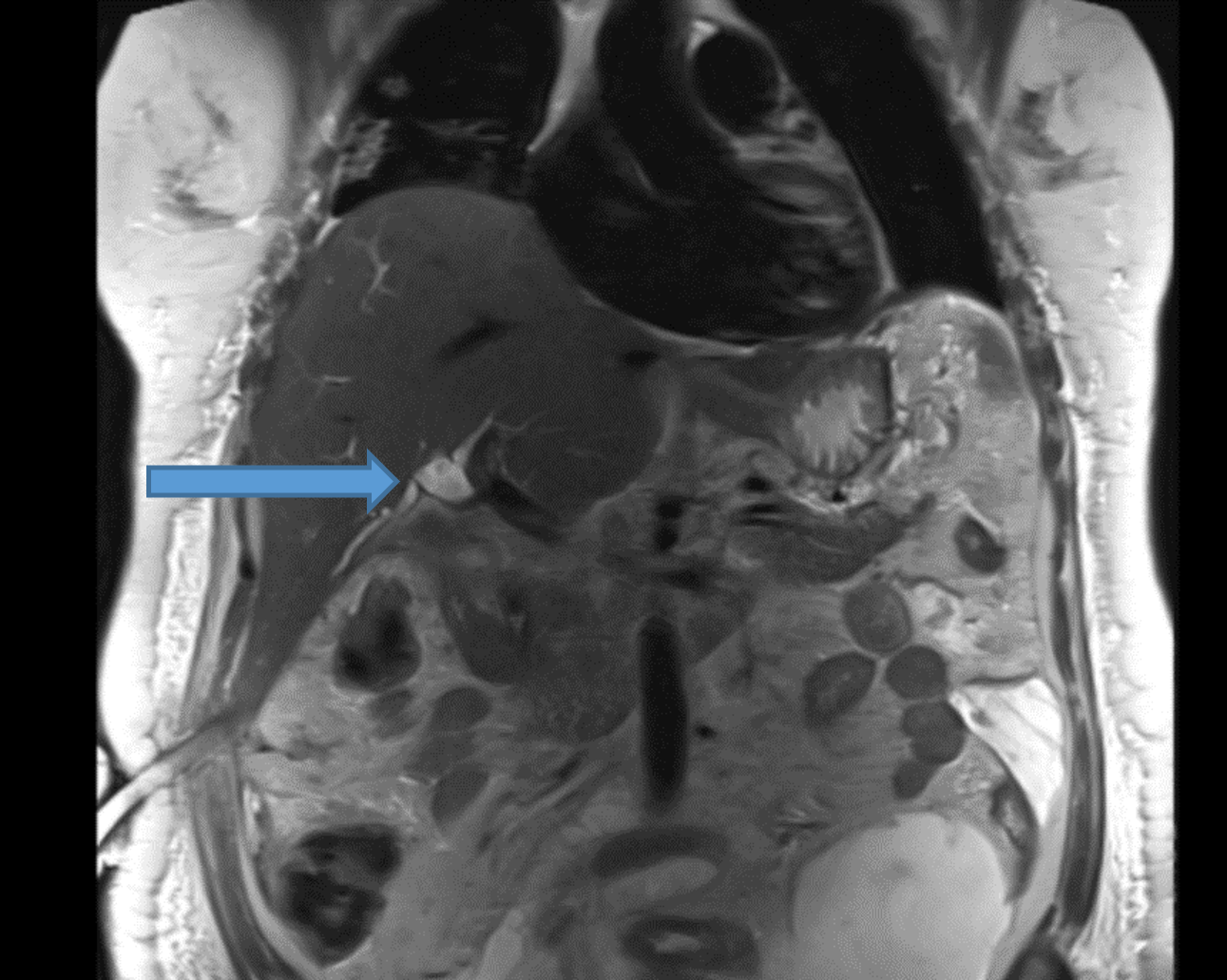
- Iatrogenic bile duct Injury post cholecystectomy– Strasberg Bismuth classification Type E2 involving common hepatic duct.
IATROGENIC BILE DUCT INJURIES
- Iatrogenic bile duct injury is a dreaded complication of cholecystectomy; estimated to occur in approximately 0.5% to 0.9% of cases.
- Early diagnosis is important for reducing morbidity and mortality.
- Ductal injuries can be caused by erroneous cutting of bile ducts, inadvertently misplaced clips, or periductal leakage of bile ducts that results in fibrosis or thermal injury.
- MRCP is a useful diagnostic test in patients suspected to have bile duct injury after surgery.
- MRCP accurately depicts the signs of stricture and excision injury and displays the anatomy completely and accurately which in turn enables to to determine appropriate treatment, whether endoscopic, percutaneous, or surgical.
STRASBERG CLASSIFICATION OF BILE DUCT INJURY
- Type A: injury to the cystic duct or from minor hepatic ducts draining the liver bed
- Type B: occlusion of the biliary tree, commonly aberrant right hepatic duct(s)
- Type C: transection without ligation of aberrant right hepatic duct(s)
- Type D: lateral injury to a major bile duct
- Type E: injury to the main hepatic duct; classified according to the level of injury
- E1 (Bismuth type 1): injury more than 2 cm from the confluence
- E2 (Bismuth type 2): injury less than 2 cm from the confluence
- E3 (Bismuth type 3): injury at the confluence; confluence intact
- E4 (Bismuth type 4): destruction of the biliary confluence
- E5 (Bismuth type 5): injury to the aberrant right hepatic duct

REFERENCES
- Kumar S, Kumar P, Chandra A. Bile duct injury: to err is human; to refer is divine.BMJ Case Rep 2019;12:e228361. doi:10.1136/bcr-2018- 228361.
- Khalid et al.Using MR Cholangiopancreatography to Evaluate Iatrogenic Bile Duct Injury.https://doi.org/10.2214/ajr.177.6.1771347.
Dr. Nikita Patel.
Cross-sectional Fellow
Manipal Hospital Radiology Group (MHRG)
Manipal Hospital, Bengaluru
Dr. Vishwanath Joshi
Consultant Radiologist.
Manipal Hospital Radiology Group (MHRG)
Manipal Hospital, Bengaluru.