
A 41-year gentleman (retroviral positive status) with severe dysarthria/dysphagia, gait ataxia.
A 41-year gentleman (retroviral positive status) with severe dysarthria/dysphagia, gait ataxia.
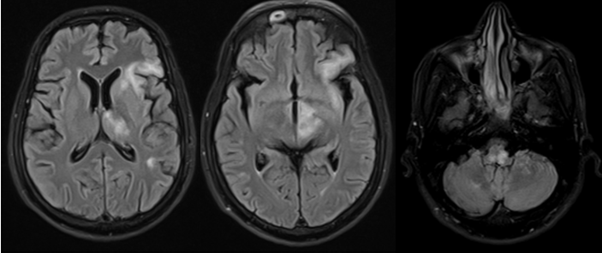
- Axial FLAIR images in contiguous sections demonstrate hyperintensities involving perisylvian left frontal and insular cortices also involving subcortical U fibers, left parietal lobe, internal capsule, thalamus, midbrain and medulla.
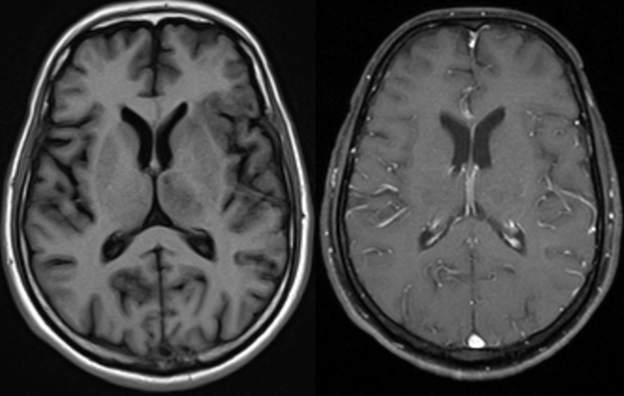
- Axial T1w precontrast and postcontrast images demonstrate no enhancement in the perisylvian left frontal and insular cortices, left parietal lobe, internal capsule, thalamus which were hyperintense on FLAIR.
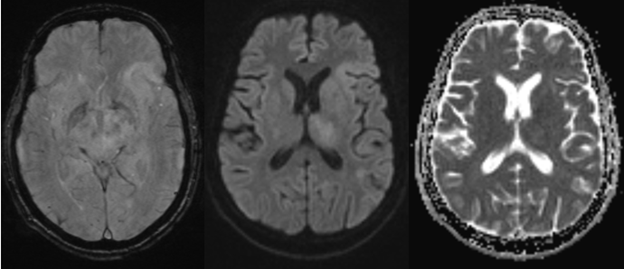
- Axial T2w GRE, DWI and ADC images demonstrate no blooming/restricted diffusion.
DIAGNOSIS:
Progressive Multifocal leukoencephalopathy.
DISCUSSION:
Progressive Multifocal leukoencephalopathy is a demyelinating disease, resulting from the re-activation of John-Cunningham virus in immunocompromised patients.
Imaging features are:
- Multifocal, asymmetric periventricular and subcortical involvement with involvement of subcortical U-fibers.
- Basal ganglia, thalamus, brainstem and cerebellum can also be involved.
- Usually does not show restricted diffusion, but may show peripheral patchy diffusion restriction at the leading edge.
- Little or no mass effect and no enhancement.
Differential diagnosis:
- Acute disseminated encephalomyelitis:
- Differing clinical history (recent infection/vaccination).
- Lesions usually enhance.
- Can show peripheral restricted diffusion.
- Involves both gray and white matter.
- HIV encephalopathy
- Has cognitive and behavioural dysfunction.
- Symmetric disease.
- Neuroparenchymal atrophy is seen.
- Sparing of subcortical U fibers and posterior fossa structures.
- Multiple Sclerosis:
- Lesion < 3 cm.
- Involvement of calloso-septal interface.
- Involvement of cortical gray matter is rare.
- Has relatively sharp border towards white matter and gray matter.
- Active lesions show enhancement.
REFERENCES:
- Wijburg MT, Witte BI, Vennegoor A, Roosendaal SD, Sanchez E, Liu Y, Jarnalo CO, Uitdehaag BM, Barkhof F, Killestein J, Wattjes MP. MRI criteria differentiating asymptomatic PML from new MS lesions during natalizumab pharmacovigilance. Journal of Neurology, Neurosurgery & Psychiatry. 2016 Oct 1;87(10):1138-45.
- Hodel J, Outteryck O, Dubron C, Dutouquet B, Benadjaoud MA, Duhin E, Verclytte S, Zins M, Luciani A, Rahmouni A, Pruvo JP. Asymptomatic progressive multifocal leukoencephalopathy associated with natalizumab: diagnostic precision with MR imaging. Radiology. 2016 Mar;278(3):863-72.
Dr. Sriram S Patwari MD, PDCC.
Consultant Radiologist and Co-lead Neuroradiology
Manipal Hospitals Radiology Group.
Dr. Vivek J. MD.
Senior Resident and Cross-sectional fellow
Manipal Hospitals Radiology Group.