
28-year-old adult brought to ER with pain at the upper part of the back and upper abdominal discomfort
- 28-year-old adult brought to ER with pain at the upper part of the back and upper abdominal discomfort
- He is a known case of APLA syndrome with recent history of treatment for LRTI- sepsis and sepsis related cholangitis
- Prior history of Deep vein thrombosis of left lower limb in 2019.
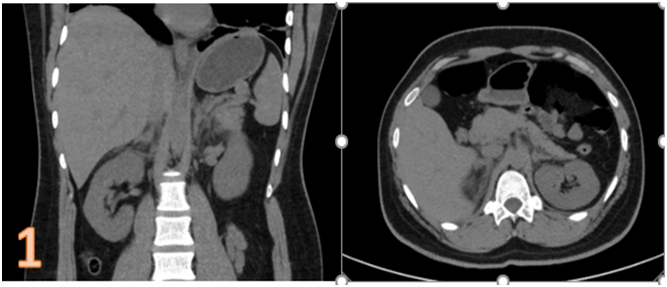
ADRENALS:
- Bilateral adrenals are diffusely bulky (arrows) (fig. 1). ?
- No distinct mass lesion seen.
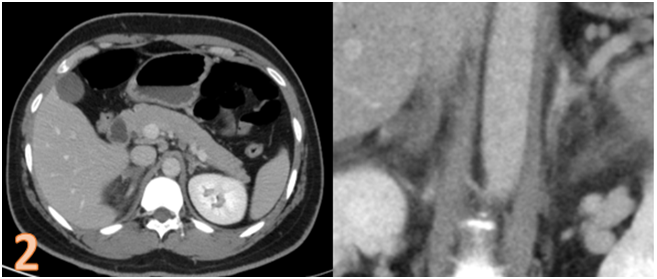
PERIADRENAL TISSUE (fig.1-2):
- Periadrenal fat stranding (*).
CONTRAST STUDY-?(fig.2):
- Non enhancing areas in body of bilateral adrenals with normal enhancement of limbs (line arrow).
DIAGNOSIS:
ADRENAL INFARCTION /HEMORRHAGE
CLINICAL SIGNIFICANCE: (1)
Antiphospholipid syndrome is an auto-immune disorder characterized by venous, arterial or small vessel thrombosis, potentially affecting multiple organ systems.
Abdominal pain1 is the said to be the most common presentation for adrenal hemorrhage / hemorrhagic infarction in these patients, which may lead to acute adrenal insufficiency.
DISCUSSION:
Adrenal Haemorrhage in Patients with Antiphospholipid Syndrome(2):
- APLA syndrome has a heterogenous group of antibodies, more commonly the lupus anticoagulant and anticardiolipin antibodies.
- Lupus anticoagulant has an anticoagulant function in vitro but has a procoagulant effect in vivo, resulting in a hypercoagulable state.
- They are associated with frequent thrombotic events, early stroke, and recurrent fetal loss in both the SLE and non- SLE populations.
- Adrenal haemorrhage is uncommon and usually preceded by other manifestations , like deep venous thrombosis as seen in our patient.
- Rarely however , adrenal haemorrhage can be the initial manifestation of the syndrome.
- The CT and MR imaging findings of adrenal haemorrhagecan be non- specific, with a high attenuationpattern or even lower-attenuation fluid in the perinephric space, similar in attenuation to the kidneys; which may representperinephric extension of adrenal haemorrhage, probably subacute.
- Early diagnosis is therefore essential for prompt management in order to address the possibility of acute adrenal insufficiency.
References:
- Aldaajani H, Albahrani S, Saleh K, Alghanim K. Bilateral adrenal hemorrhage in antiphospholipid syndrome. Anticoagulation for the treatment of hemorrhage. Saudi Med J. 2018;39(8):829-833. doi:10.15537/smj.2018.8.22437
- https://radiopaedia.org/articles/antiphospholipid-syndrome?lang=us
- Provenzale JM, Ortel TL, Nelson RC. Adrenal hemorrhage in patients with primary antiphospholipid syndrome: imaging findings. AJR Am J Roentgenol. 1995 Aug;165(2):361-4. doi: 10.2214/ajr.165.2.7618557. PMID: 7618557.
Dr Sunita Gopalan
DMRD, FRCR
Senior Consultant Radiologist
Columbia Asia Radiology Group
Dr Naveen SS,
Cross-Sectional Imaging Fellow
Columbia Asia Radiology Group