A 46 year old female with history of Urinary tract infection –MDR pseudomonas treated with antibiotics. Now presented with severe abdominal pain and vomiting.
HISTORY
- A 46 year old female with history of Urinary tract infection –MDR pseudomonas treated with antibiotics. Now presented with severe abdominal pain and vomiting.
- CECT Abdomen and pelvis advised.
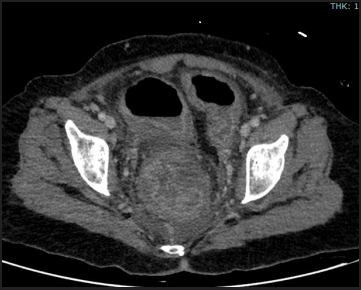
A.CECT ABDOMEN AND PELVIS
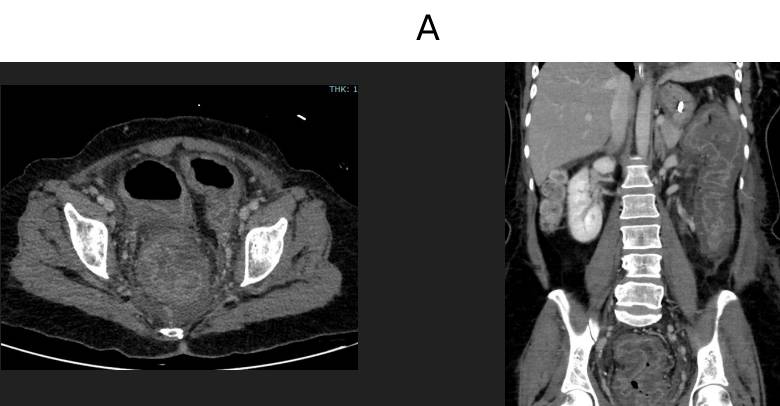
B.CECT ABDOMEN AND PELVIS
LEGENDS :
- A. Diffuse circumferential colonic wall thickening involving the descending colon, sigmoid and rectum with submucosal edema. Mild thickening of the haustral folds noted.
- B. Diffusely air filled distended colonic loops and rectum, maximum diameter reaching ~ 6 cm.
DIAGNOSIS
PSEUDOMEMBRANOUS COLITIS
DISCUSSION
- Acute inflammatory colitis caused by toxins of Clostridioides difficile
- Characterized by pseudomembrane formation over colonic mucosa
Why Important?
- Most common cause of antibiotic-associated colitis
- Can progress to toxic megacolon, perforation, sepsis
- Increasing incidence in hospitalized patients
ETIOLOGY AND RISK FACTORS Causative Organism
- Clostridioides difficile
- Anaerobic, spore-forming Gram-positive bacillus
Pathogenesis Trigger
- Broad-spectrum antibiotics: Clindamycin, Cephalosporins, Fluoroquinolones, Carbapenems
Risk Factors
- Recent hospitalization
- ICU stay
- Elderly (>65 years)
- Immunocompromised
- PPI use
- Post abdominal surgery
PATHOLOGY Mechanism
- Antibiotics → Altered gut flora
- C. difficile overgrowth
- Production of:
- Toxin A (enterotoxin)
- Toxin B (cytotoxin)
Pathological Changes
- Mucosal epithelial necrosis
- Neutrophilic infiltration
- Fibrin + mucus + inflammatory cells form: Yellow-white pseudomembranes
Distribution
- Usually diffuse
- May involve entire colon (pancolitis)
- Rectum often involved (helps differentiate from ischemic colitis)
INTRA OPERATIVE IMAGES 
- Yellowish white psudomembrane
LAB FINDINGS  CT FINDINGS
CT FINDINGS
- Diffuse colonic wall thickening
- Often >10 mm
- More than other colitides
- Accordion Sign
- Oral contrast trapped between edematous haustra
- Thumbprinting
- Submucosal edema
- Target / Double halo sign
- Mucosal hyperenhancement + submucosal edema
- Pericolonic fat stranding
- Often mild relative to wall thickening
- Ascites (common)
COMPLICATIONS
- Toxic megacolon
- Bowel perforation
- Sepsis
- Multiorgan failure
- Recurrence (20–30%)
MANAGEMENT First Line
- Oral vancomycin
- Fidaxomicin
Severe Cases
- IV metronidazole (adjunct)
- Surgery (subtotal colectomy) in toxic megacolon
DR. ANITA NAGADI
SENIOR CONSULTANT RADIOLOGIST,
MANIPAL HOSPITAL, YESHWANTHPUR
DR. FATHIMATH ASHILI KM
RADIOLOGY RESIDENT,
MANIPAL HOSPITAL, YESHWANTHPUR