
53years old female come with history of cough with shortness of breath since 6 days associated with fever. She is a known case of retroviral disease.
- 53years old female come with history of cough with shortness of breath since 6 days associated with fever. She is a known case of retroviral disease.
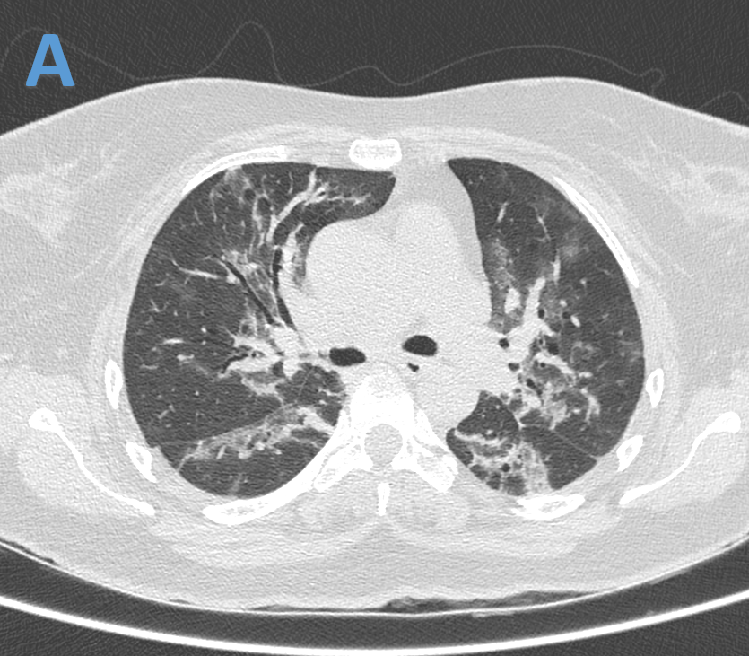
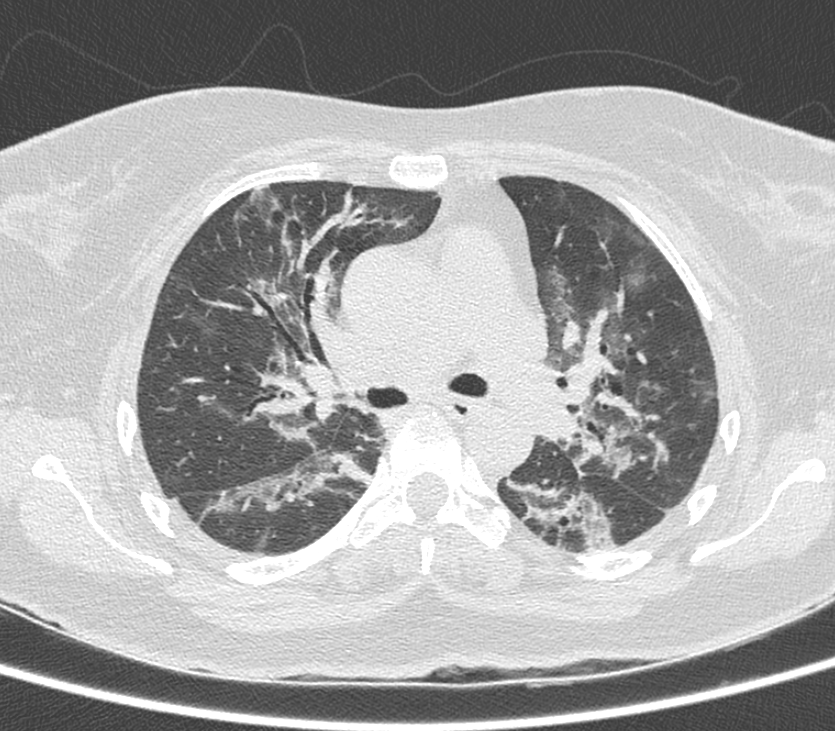
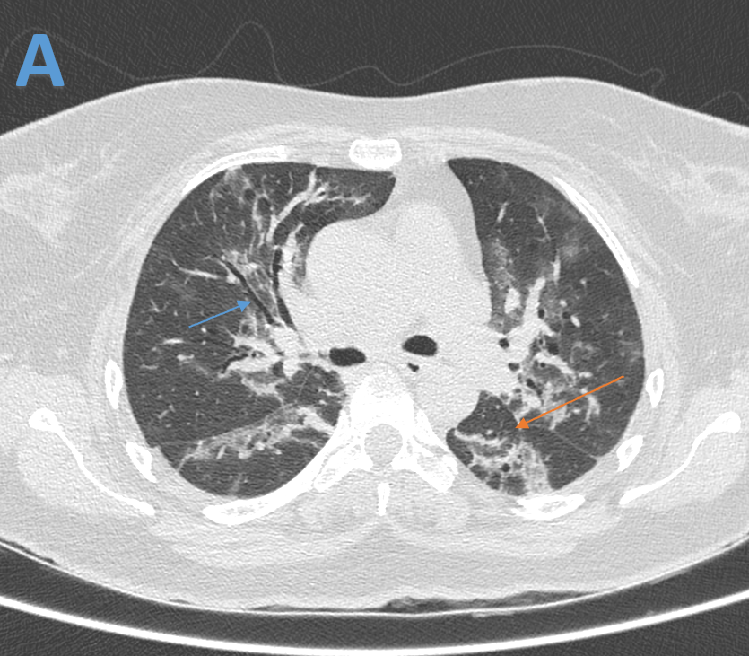
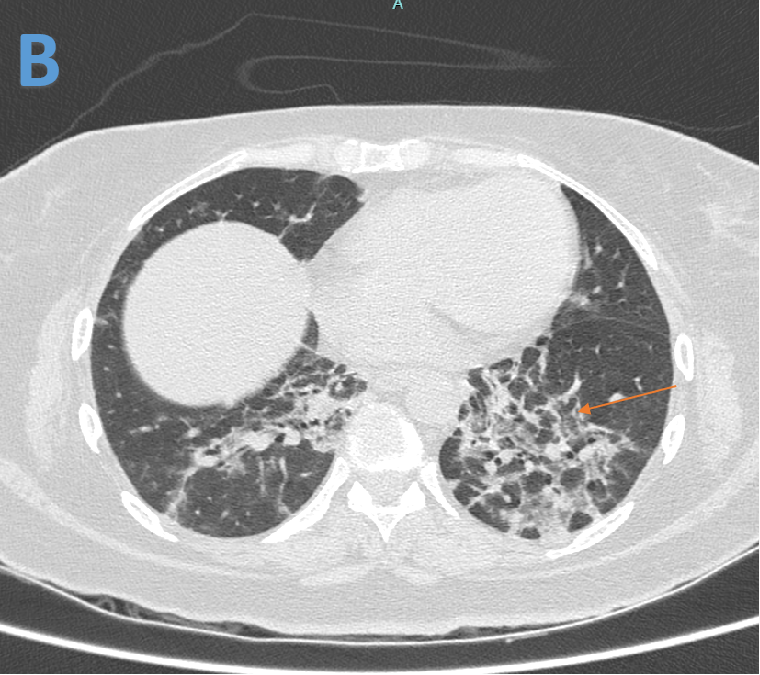
- Patchy areas of fibrotic changes(orange arrow) with bronchiolectasis(blue arrow) in perihilar and peribronchiovascular distribution associated with ground glass opacities
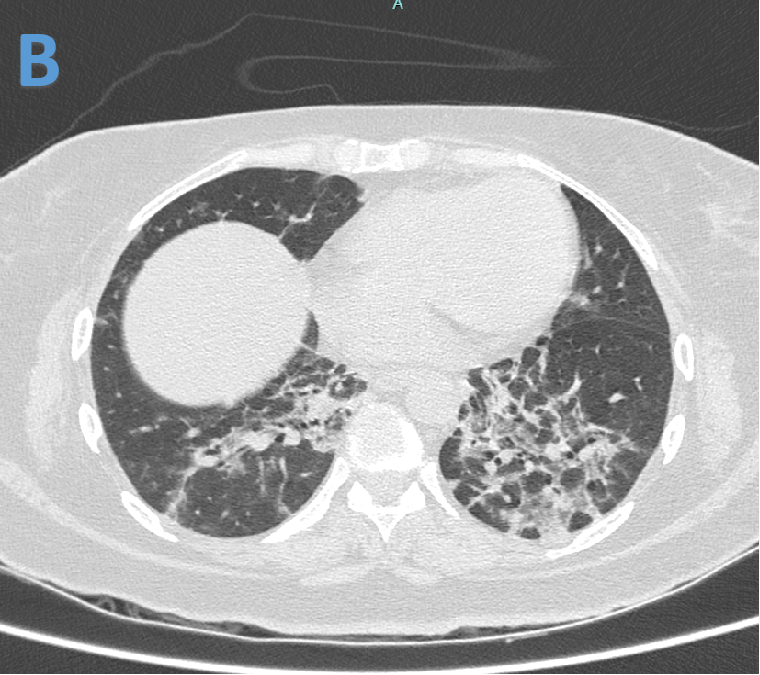
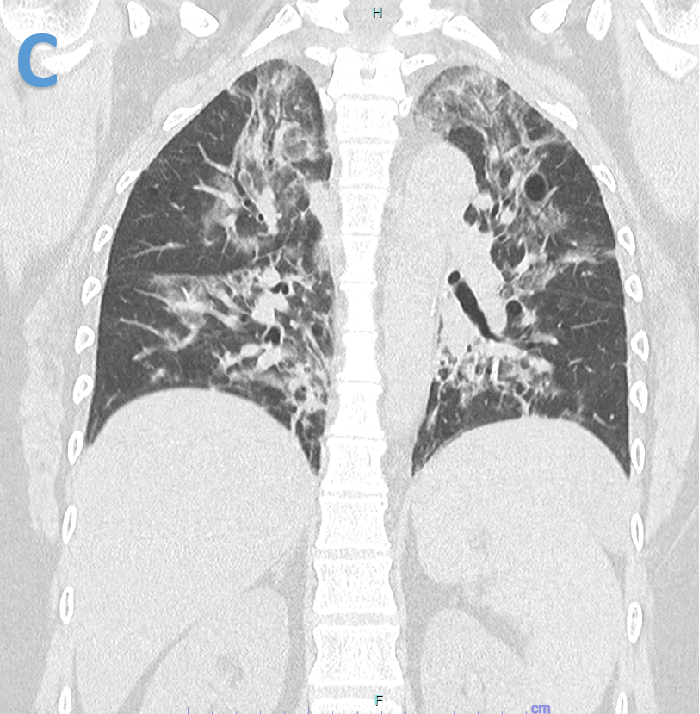
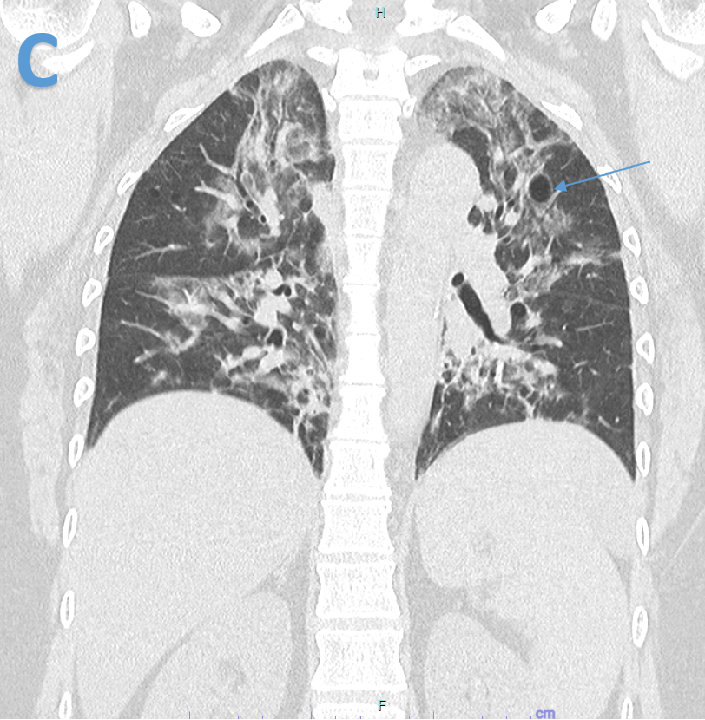
- Fibrotic changes with areas of ground glass opacities and lung cyst(blue arrow) in central distribution.
DIAGNOSIS:
- Pneumocystis jirovecii pneumonia.
DISCUSSION:
Pneumocystis jirovecii pneumonia
- Pneumocystis jirovecii pneumonia (PCP) is said to be caused by pneumocystis jirovecii (formerly pneumocystis carinii) an ubiquitous protozoan which is classified as a fungus.
- PCP is the most common pulmonary infection in patients with AIDS and the most frequently used index to diagnose AIDS in the industrialized world. Even the first episode can be severe with a high mortality rate (up to 25%).
- PCP occurs mainly in immunocompromised patients and especially in patients with the Acquired Immuno Deficiency Syndrome (AIDS). The maximal risk exists when the CD4+ count is less than or equal to 200 cells per cubic millimetre.
Clinical features:
- The clinical symptoms of PCP are non-specific and variable in their presentation like non-productive cough, dyspnea, shortness of breath, and fever. The clinical course at the onset of infection is also variable. It can be insidious or brutal with a great alteration of the clinical status.
Imaging
- PCP has a large spectrum of radiological and CT features. Classical X ray signs include diffuse or perihilar, bilateral, symmetric, reticular or granular infiltrates that can be exclusively interstitial or associated with air-space consolidation.
- The classical CT pattern is an extensive ground-glass attenuation, homogeneous or patchy in its presentation, sometimes associated with a thickening of the septal lines. However, atypical features are more frequently encountered and must be known. These findings include cavitating nodules or masses, cysts, spontaneous pneumothorax, focal alveolar or lobar consolidation, miliary nodular pattern, and interstitial fibrosis (in the chronic form of PCP).
- Mediastinal and hilar lymph node enlargement, and pleural effusions can also be seen, but differential diagnosis in cases such as mycobacterial and bacterial infections, lymphoma and Kaposi’s sarcoma should be excluded. PCP may present as an upper lobe distribution, simulating tuberculosis especially in patients with AIDS treated with prophylactic inhaled pentamidine.
- The cystic form of PCP is encountered in 10%–30% based on different studies. The cysts are often multiple, varying in size and location.
Reference
- Crans CA Jr, Boiselle PM.Imaging features of Pneumocystis carinii pneumonia. Crit Rev Diagn Imaging. 1999 Aug;40(4):251-84. (PMID: 10514937)
- Vasseur R, Genevois A, Dacher JN, Thiebot J. Cystic pneumocystis jirovecii pneumonia. Eurorad, ISSN: 1563-4086
Dr Pravin kumar M
MBBS, DMRD, DNB
Senior Consultant Manipal Hospitals Radiology Group Hebbal.
Dr Vasanth kumar L
MBBS, M.D.
Cross section imaging fellow - MHRG

