79 year old gentleman, known hypertensive and diabetic, post CABG, with asymptomatic splenomegaly and intestinal obstruction in 2015 (managed conservatively). Now presented with pain abdomen since 2-3 days. Patient was on NSAIDS on and off, stopped recent
79 year old gentleman, known hypertensive and diabetic, post CABG, with asymptomatic splenomegaly and intestinal obstruction in 2015 (managed conservatively). Now presented with pain abdomen since 2-3 days. Patient was on NSAIDS on and off, stopped recently.




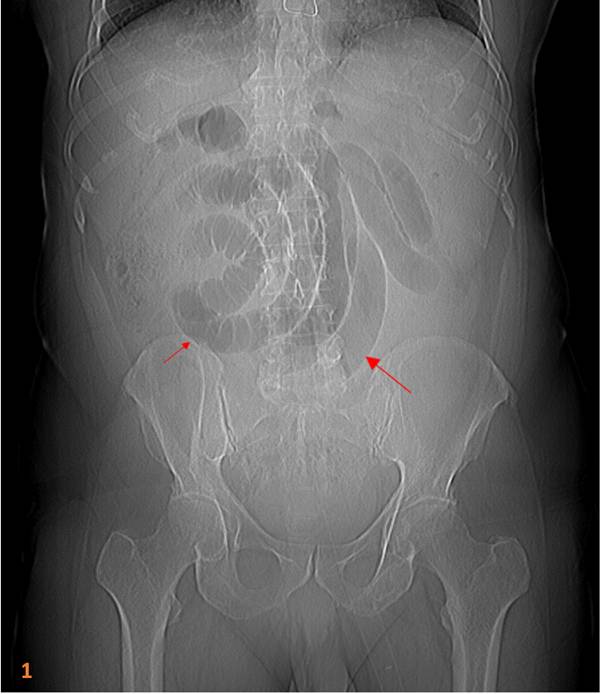
- CT topogram demonstrates dilated distal jejunal and ileal loops (Fig 1).
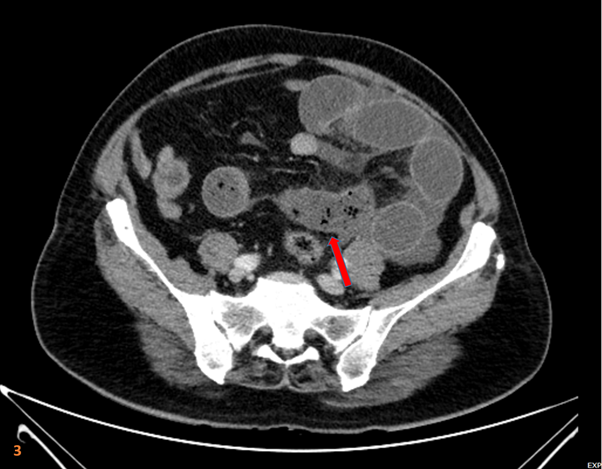
- CECT abdomen: Focal short segment circumferential wall thickening in a loop of ileum with stratified enhancement (Red arrow in figure 2).
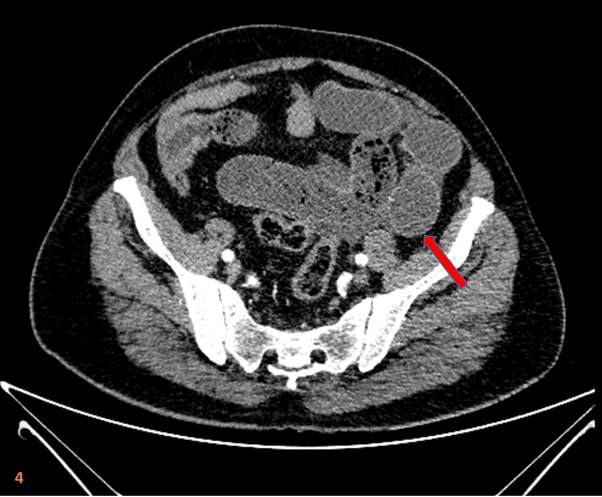
- Resultant upstream dilatation of the proximal ileal loops with small bowel faeces sign with fluid around bowel loops and mesenteric edema (Red arrows in figure 3 and 4) – suggestive of acute small intestinal obstruction.

Diagnosis:
NSAID induced enteropathy.
Discussion:
- Nonsteroidal anti-inflammatory drugs can lead to gastrointestinal tract ulcers and small bowel mucosal diaphragms (thin weblike strictures) – known as small bowel diaphragm disease.
- NSAIDs can result in injury to the gastrointestinal tract due to their inhibition of prostaglandin, which impairs gastrointestinal mucosal defense mechanisms. This injury commonly manifests as ulcers in the stomach and proximal duodenum and can cause mucosal diaphragms in the small bowel, especially the ileum. Areas of inflammation can then hemorrhage, form granulation tissue, and eventually result in weblike mucosal strictures.
- Thus, in a patient with longterm NSAID use and unexplained small bowel obstruction, mucosal diaphragms causing obstruction should be considered in the differential diagnosis.
- Imaging findings of NSAID induced enteropathy are:
- Focal intraluminal web or diaphragm at the site of stricture that can lead to marked luminal narrowing.
- Imaging differentials include:
- Crohn disease: Longer segments of transmural involvement
- Ischemic enteritis: Bowel wall thickening; strictures can be late result.
- Radiation enteritis: Longer strictures; pelvic SB segments.
- The imaging features that differentiate diaphragm disease from Crohns disease include:
- Clinical presentation does not typically include diarrhea
- It never involves the terminal ileum
- Mucosal hyper-enhancement is variably encountered
- There is a predominance of focal strictures rather than long segment disease
- Bowel wall symmetry is preserved.
REFERENCES:
- Flicek KT, Hara AK, Petris GD, Pasha SF, Yadav AD, Johnson CD. Diaphragm disease of the small bowel: a retrospective review of CT findings. American Journal of Roentgenology. 2014 Feb;202(2):W140-5.
- Raju SE, Singh R, Raju M. NSAID enteropathy: a review of the disease entity and its distinction from Crohn’s enteropathy. Journal of Gastrointestinal and Abdominal Radiology ISGAR Vol. 2019;2(2).
Dr. Suvarna Kote
Radiology resident- Manipal Hospitals Radiology Group.
Dr. Sunita Gopalan
DMRD, FRCR
Senior Consultant Radiologist
Manipal Hospitals Radiology Group.