A 47-year-old presented with haemoptysis and cough for one week and breathing difficulties for ten years
A 47-year-old presented with hemoptysis and cough for one week and breathing difficulties for ten years.

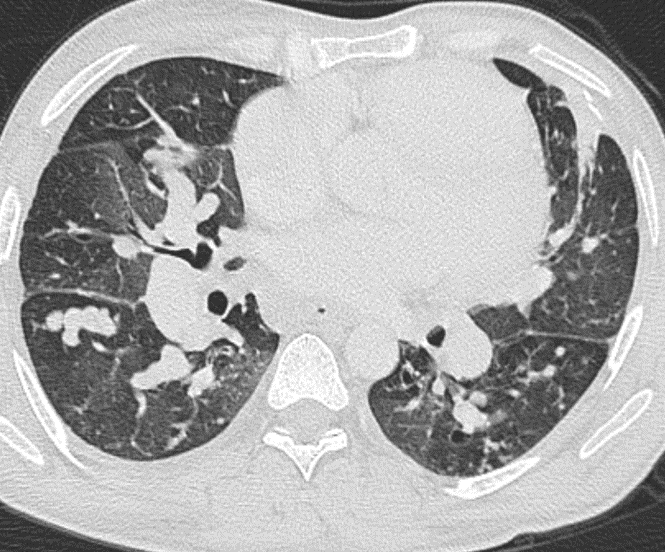
A: Axial HRCT lung window images shows – Severe aneurysmal dilatation of multiple pulmonary lobar and segmental branches in bilateral lungs (red arrows) with normal-sized bronchus. Mild cardiomegaly.
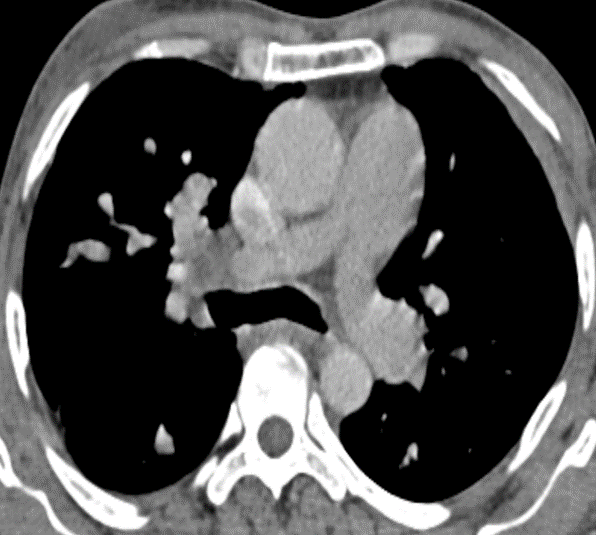
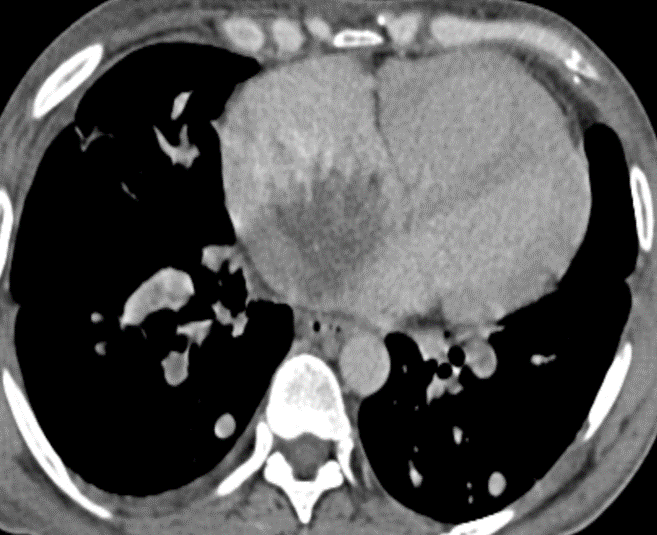
B: Axial HRCT mediastinal window images show There is a hypodense hypo-enhancing soft tissue density lesion in the right atrium (blue arrow) along the inter-atrial septum. Small speck of calcification is seen within this lesion (yellow arrow). Normal-sized main pulmonary artery (red arrow).
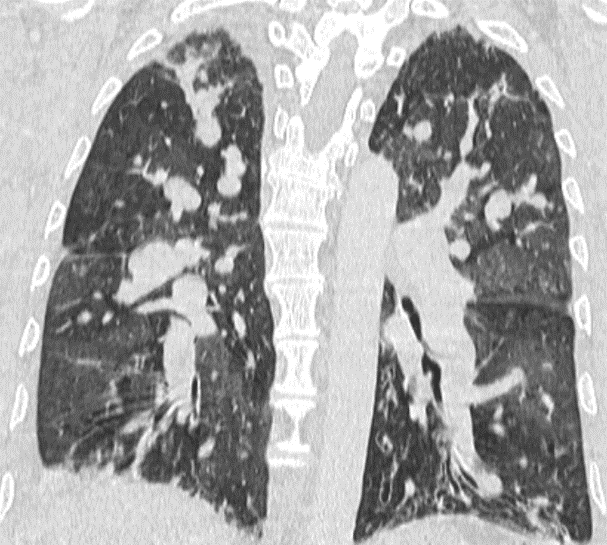
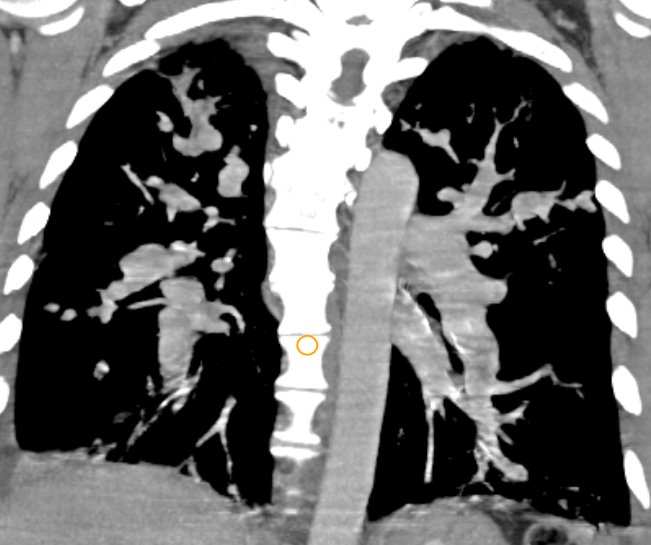
C: Coronal lung and mediastinal window images show – Severe aneurysmal dilatation of multiple pulmonary lobar and segmental branches in bilateral lungs (red arrows) with normal size bronchus.
Diagnosis : Right atrial myxoma with pseudo-aneurysms of the lobar and segmental pulmonary arteries.
DISCUSSION:
- Multiple pulmonary aneurysms are rare and their etiology is not clear. We present a case of a right atrial cardiac myxoma (CM) and multiple peripheral pulmonary arteries aneurysms (PAA).
- Two reports exist in literature reporting the occurrence of PAA in association with a right?sided CM—one based on the postmortem examination and the other in a 48?year?old woman.
- The aneurysm formations can be attributable to the CM cells.
- Contingent on the histopathological examination, we hypothesize that the myxoma cells have inherent potential to invade and transgress native tissue of the vascular wall (akin to metastatic cells) causing weakness and dilation of the pulmonary arteries.
- Systemic emboli are described in patients of left?sided CM frequently, along with subsequent evolution of cerebral aneurysms formed in its association.
- In cases of right CM, however, the importance of pulmonary emboli is underestimated.
- Histological examination showed that the emboli inside the lung arterioles were comprised of distinctive myxoma cells in syncytial groups.
- These cells were not just limited to the intraluminal space but were also found inside the arteriolar wall and the pulmonary parenchyma.
- The distant spread of CM cells to the lungs, their invasion, and subsequent transgression of the vessel wall vindicate the hypothesis that these “histologically benign” cells have an inherent potential for metastases.
- It is then, within plausibility, to infer that these cells might become the seedlings for a future recurrence.
- The aneurysm formation is understood as consequent to the weakening of the arterial walls through invasion circumstantiating the causal relationship between CM and PAAs.
- Computed tomography angiography (CTA) of the thorax shows multiple fusiform and saccular dilatations of bilateral peripheral pulmonary arteries, some of them with an intraluminal thrombus.
- Peripheral venous thromboses needs to be excluded using doppler sonography and magnetic resonance (MR) angiography.
- To evaluate for the presence of malignancy, a positron emission tomography?MR imaging was performed, which may reveal moderate uptake by the mass in the right atrium and minimal absorption by the aneurysms.
- Oncological therapy with chemotherapy and/or radiotherapy could not be justified, as histologically this tumor is proven benign (low Ki?67 index levels). IL?6 levels, alongside being responsible for the constitutional symptoms and immunological abnormalities, are a known marker for recurrence.
- Downregulation of IL?6 expression through molecular targeting (miR?217) has been shown to arrest the proliferation of CM cells.
- A long?term vigilance, as a part of our “wait?and?watch” strategy requisite with imaging (CTA and echocardiography) and serum IL?6 levels, is the prudent course to take.
References
- Geddes DM, Kerr IH. Pulmonary arterial aneurysms in association with a right ventricular myxoma. Br J Radiol. 1976;49:374?376.
- Dong A, Lu J, Zuo C. Multiple peripheral pulmonary artery aneurysms in association with a right atrial myxoma. Circulation. 2016;133: 444?446.
- Attum AA, Johnson GS, Masri Z, Girardet R, Lansing AM. Malignant clinical behavior of cardiac myxomas and “myxoid imitators”. Ann Thorac Surg. 1987;44:217?222.
- Mendoza CE, Rosado MF, Bernal L. The role of interleukin?6 in cases of cardiac myxoma: clinical features, immunologic abnormalities, and a possible role in recurrence. Tex Heart Inst J. 2001;28:3?7.
- Zhang J, Wang C, Xu H. miR?217 suppresses proliferation and promotes apoptosis in cardiac myxoma by targeting interleukin?6. Biochem Biophys Res Commun. 2017;26(490):713?718.
Dr. PRAVEEN WALI,
Senior Consultant Radiologist
Manipal Hospital, Yeshwanthpur, Bengaluru.Dr. VAIBHAV BHANDARI
Senior resident, Radiologist
Manipal Hospital, Yeshwanthpur, Bengaluru.