A 27 year old lady presenting with dysphagia, and with history of partially treated tonsillitis
A 27-year-old lady presenting with dysphagia, and with history of partially treated tonsillitis
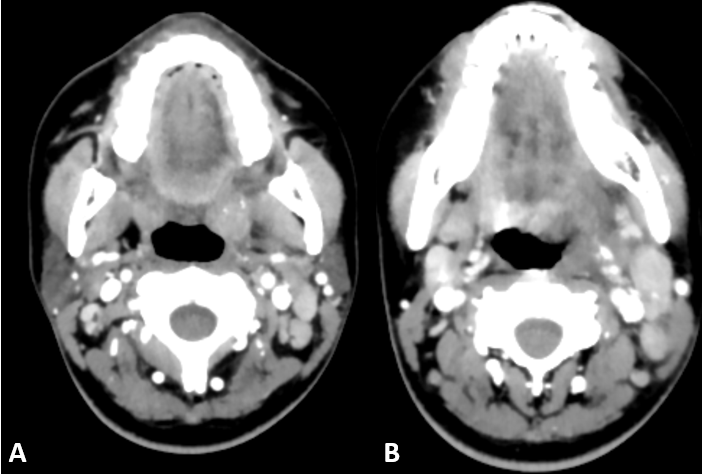
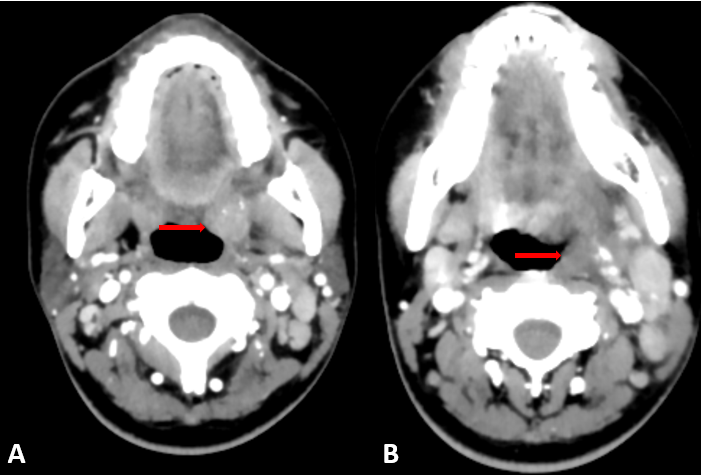
- Enlarged and edematous left tonsil with fluid collection in the left tonsillar fossa and the left tonsillar
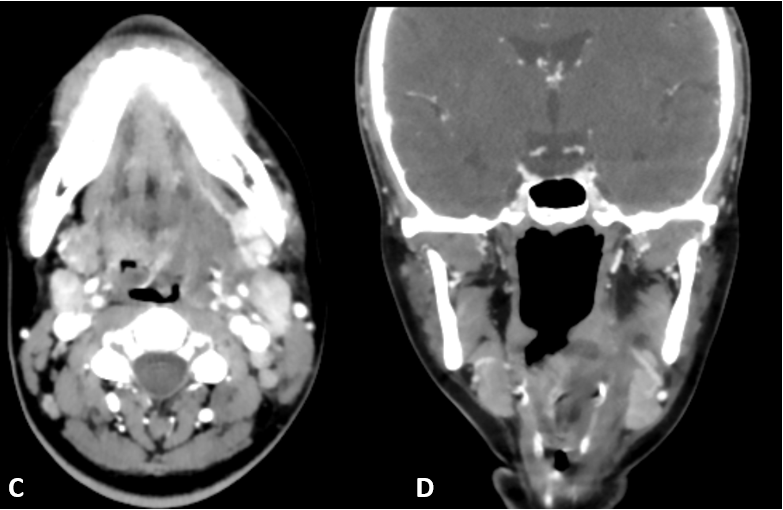
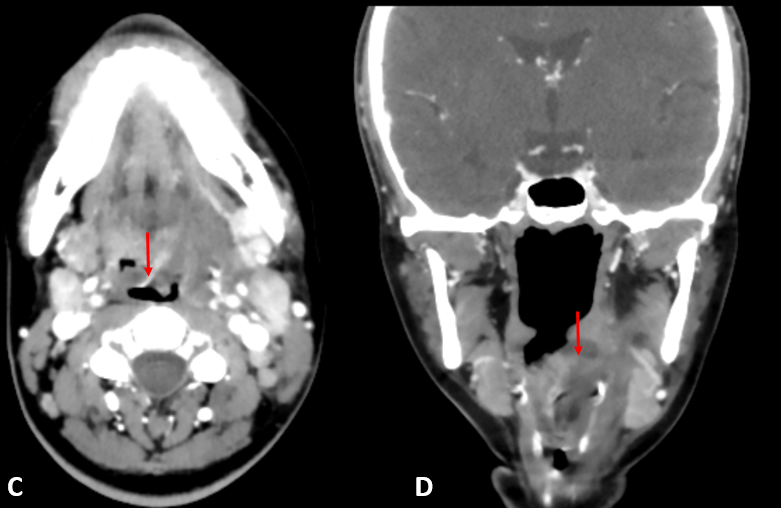
- At the level of the oropharynx, there is significant luminal compromise. The collection and edema extend to involve the left para-laryngeal soft tissues and the left vocal cord.
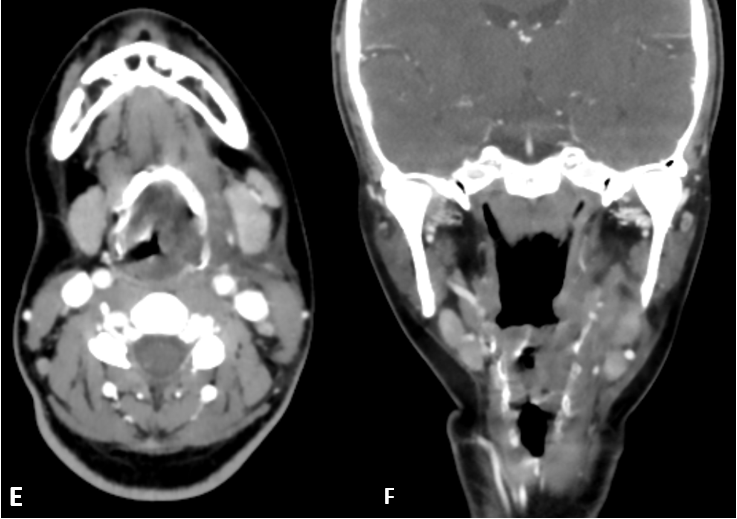
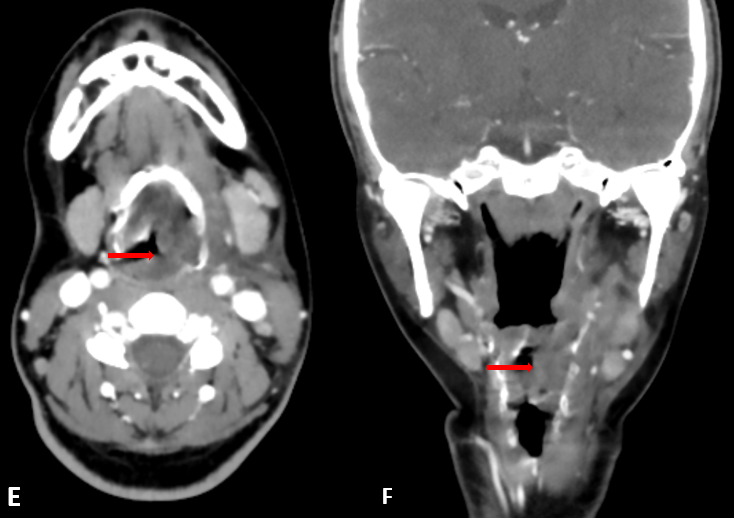
- Extension of fluid with mass effect into the left parapharyngeal space and along the left lateral wall of the oropharynx and hypopharynx up to the level of the cricoid.
DIAGNOSIS:
- Left peritonsillar abscess (Quinsy) with extensive extension into the left parapharyngeal space.
Discussion:
- Patients often present to the emergency department with a wide variety of nontraumatic infectious, inflammatory, and neoplastic conditions of the head and neck.
- Potentially life-threatening conditions include
- Oral cavity infections
- Tonsillitis and peritonsillar abscess
- Sialadenitis & parotiditis
- Thrombophlebitis
- Periorbital and orbital cellulitis
- Infectious cervical lymphadenopathy.
- Less common conditions include epiglottitis, invasive fungal sinusitis, angioedema, and deep neck abscess
- Modalities for diagnosis:
- Ultrasound has low sensitivity for deep neck infections; however can be utilized in emergency setting.
- CT is the first-line imaging modality in the emergency setting.
- Magnetic resonance imaging plays an important secondary role due to superior soft-tissue contrast.
- Routes of spread:
- Tonsillitis suppurates and internally cavitates to create an intratonsillar abscess; however, a true tonsillar abscess is rare.
- The infection penetrates the tonsillar capsule and the peritonsillar space—a potential space between the tonsillar capsule and the superior constrictor muscle
- The infection may then continue to extend into the parapharyngeal, masticator, or submandibular space.
- The resulting peritonsillar cellulitis resolves over several days; however, if it goes untreated, a peritonsillar abscess develops, typically along the superior tonsillar pole.
Imaging features
- Ultrasound features
- Mild hypoechoic collection is anteromedial to the internal carotid artery.
- Probe pressure may elicit movement of the debris within the abscess
- Color flow or power Doppler may demonstrate circumferential hyperemia.
- CT features peritonsillar cellulitis
- Tonsillar enlargement
- Linear, striated enhancement of the palatine tonsils and posterior pharyngeal soft tissues
- Medial apposition of the enlarged tonsils resulting in a “kissing tonsils” appearance.
- Central liquefaction surrounding him like enhancement is diagnostic of peritonsillar abscess.
- Fluid collection dissecting along multiple planes as in our case.
REFERENCES:
- Emergency Imaging Assessment of Acute, Nontraumatic Conditions of the Head and Neck Erin Frankie Capps, James J. Kinsella, Manu Gupta, Amol Madhav Bhatki, and Michael Jeffrey Opatowsky. RadioGraphics 2010 30:5, 1335-1352
- Ong YK, Goh YH, Lee YL. Peritonsillar infections: local experience. Singapore Med J. 2004;45 (3): 105-9.
Dr. Sushant Mittal MD
Cross-sectional Fellow
Columbia Asia Radiology Group.
Dr Anita Nagadi MD, MRCPCH, FRCR
Senior Consultant Radiologist
Columbia Asia Radiology Group.