30-year-old gentleman with anterior knee pain from 2 weeks. History of knee injury 1 month back
A 30-year-old gentleman with anterior knee pain for 2 weeks. History of knee injury 1 month back.

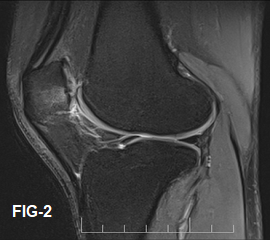
- Sagittal T2WI (Fig.1) and PDFS (Fig.2) demonstrate thickened, disorganized, and edematous infrapatellar plica, with mild edema of the surrounding Hoffa fat pad. The note is made of subchondral marrow edema in the patella.
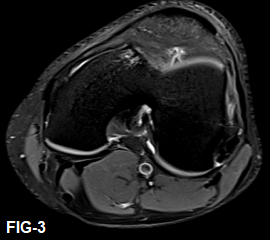
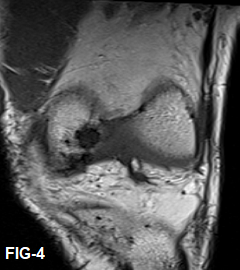
- Axial PDFS (Fig.3) and coronal T1WI (Fig.4) demonstrate the same findings. The note is made of subchondral edema/cysts in the lateral facet of the Trochlea.
DIAGNOSIS:
- Sprain of Infrapatellar plica
DISCUSSION:
- Plicae are the embryonic mesenchymal remnants in the lining of joints. Four plicae have been described in knee based on location – Suprapatellar, infrapatellar, medial and lateral.
- The infrapatellar plica (also known as ligamentum mucosum) is the most frequently seen knee plica at arthroscopy.
- It courses anteriorly and inferiorly from femoral origin anterior to the ACL, courses parallel to the ACL into the infrapatellar fat pad, then curves upward through the infrapatellar fat pad to attach to the inferior patella.
- On MR imaging, normal infrapatellar plicae are thin and often difficult to distinguish from the adjacent ACL. A normal cleft in the infrapatellar fat pad is commonly seen just below the infrapatellar plica, known as the horizontal cleft of the infrapatellar fat pad or ligamentum mucosum recess.
MR imaging features:
- A thickened, irregular infrapatellar plica on MRI suggests inflammation or previous injury.
- Acute injury of the infrapatellar plica may cause edema within the plica and surrounding infrapatellar fat pad in a characteristic curvilinear pattern, following the course of the plica.
- Plica may be symptomatic without injury with similar findings as acute sprain.
- Other less frequent complications of knee plicae includes chondral injury and compartmentalization.
- Care should be taken not to mistake anteromedial meniscofemoral ligament with infrapatellar plica. This structure courses anterior to ACL but does not traverse through infrapatellar fat pad.
- Sprain of knee plicae are not uncommon and are often overlooked causes of anterior knee pain.
- Reporting checklist must include assessment of knee plicae in cases of unexplained anterior knee pain.
Dr Vivek J, MD
Senior resident & Cross Section fellow
MHRG
Dr. Dayananda Sagar G, MD
Consultant radiologist
MHRG