26 year old female with previous history of right sided otitis externa and otitis media, post-operative status. Now complaints of right sided conductive hearing loss
26-year-old female with a previous history of right-sided otitis externa and otitis media, post-operative status. Now complaints of right-sided conductive hearing loss


FINDINGS
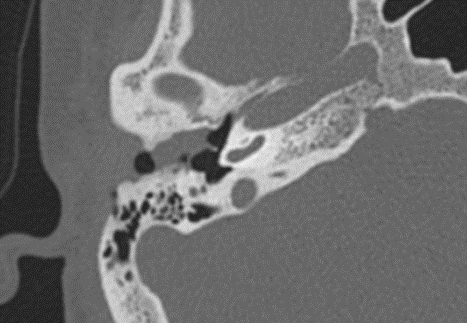
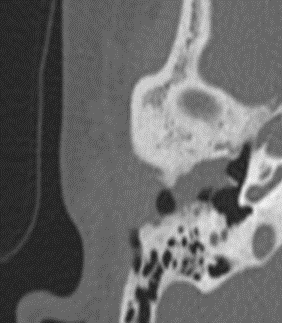
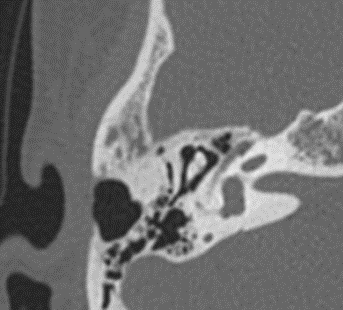
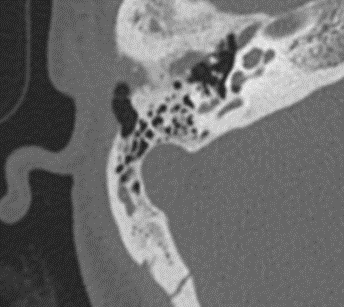
- Opacification is noted in the right external auditory canal measuring 11 x 5 mm. The opacification is contiguous with the right tympanic membrane. Mild erosions were noted in the anterior and posterior walls of the external auditory canal.
- Previous cortical mastoidectomy.
The ossicular chain appears normal.
No blunting of scutum.
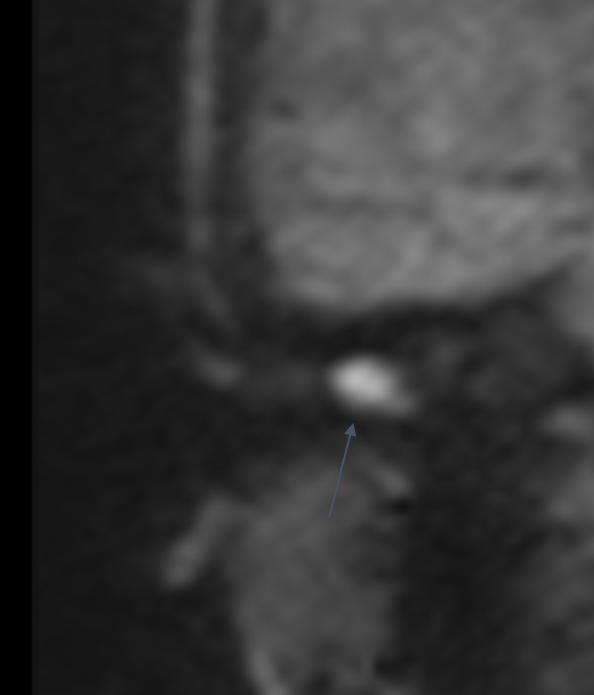
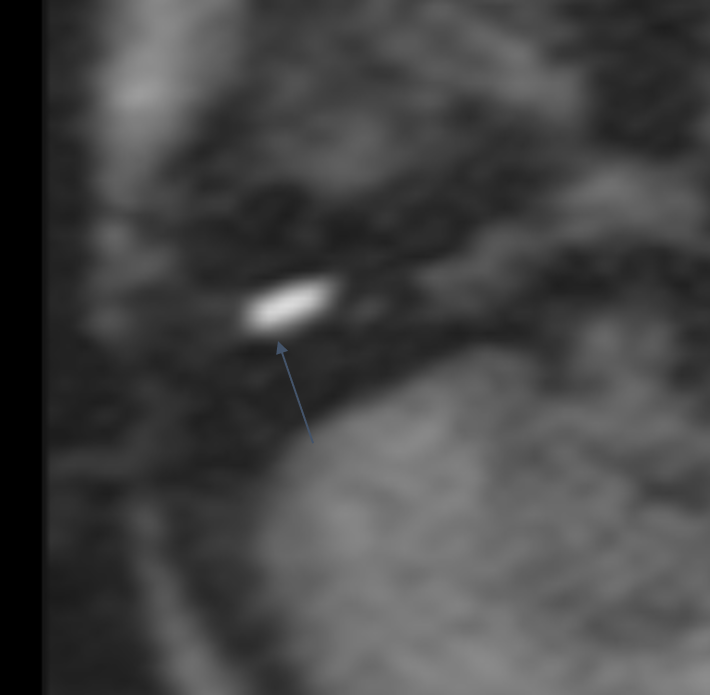
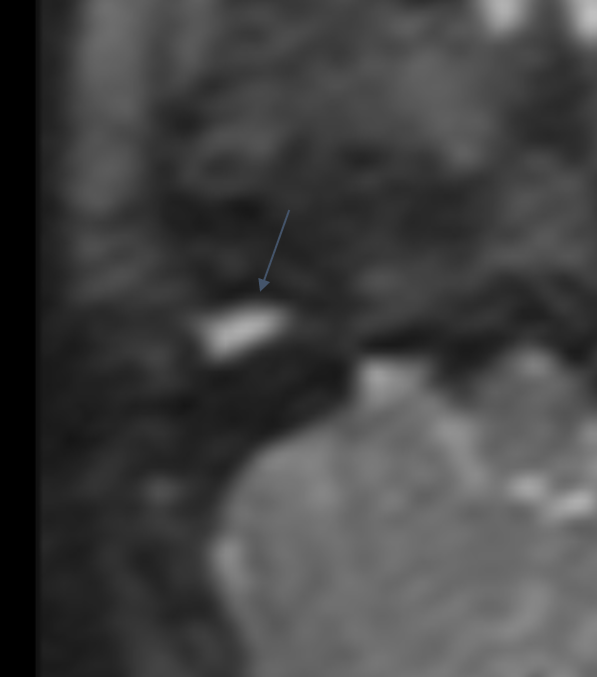
Erosions were noted in the superior wall of the external auditory canal. - The MRI demonstrates a 10 x 4 x 6 mm focus of restricted diffusion corresponding to the opacification in the right external auditory canal.
DIAGNOSIS:
Features are in keeping with RIGHT external auditory canal cholesteatoma. No attic or mastoid involvement.
DISCUSSION:
- With high-resolution temporal bone CT examination, external auditory canal cholesteatoma is most commonly seen as an EAC soft-tissue mass with associated bone erosion and intramural bone fragments. The bone erosion adjacent to the soft-tissue mass may be smooth, similar to a middle ear cholesteatoma; however, the erosion may be irregular secondary to the necrotic bone and periostitis. Usually, the inferior and/or posterior walls are involved [1]
Classification[3]
External auditory canal cholesteatoma can be divided into:
- Primary (idiopathic/spontaneous): Rare. No antecedent cause identified.
- Secondary: More common. Postoperative, postinflammatory, posttraumatic, radiation-induced.
- A special type of secondary cholesteatoma of the external auditory canal are those associated with congenital atresia of the external auditory canal.
An external auditory canal cholesteatoma can be mimicked by many conditions like keratosis obturans, carcinoma etc, computed tomographic imaging of the temporal bone is useful in arriving at the correct diagnosis, to determine the extent of the lesion and the bony involvement.[2]
The imaging differentials include keratosis obturans and mycetoma. Keratosis obturates is a pathological condition characterized by the accumulation of desquamated keratin in the external auditory meatus. The features that made keratosis obturans less likely were the chronic history and the irregular bony erosions instead of the smooth scalloping seen in keratosis.
REFERENCES
[1] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8148678/
[2] https://www.eurorad.org/case/17326
[3]radiopaedia.org/articles/external-auditory-canal-cholesteatoma.
Dr. ANITA NAGADI
Senior Consultant radiologist.
Lead Head and neck onco-imaging Manipal Hospital.
Yeshwanthpur, Bengaluru.
Dr. M MATHEW JAMES
Radiology resident
Manipal Hospital, Yeshwanthpur, Bengaluru.